
Post written by Kyoko Wada, MD, MA, PhD, and Michael J. Szego, MHSc, PhD, from the Centre for Clinical Ethics, Providence Healthcare, St. Joseph’s Health Centre, St. Michael’s Hospital Network, and the Department of Family and Community Medicine, Dalla Lana School of Public Health, Joint Centre for Bioethics, University of Toronto, Toronto, Canada.


Based on a clinical ethics consultation, we examined whether a do-not-resuscitate (DNR) order should be revisited by the gastroenterologist prior to endoscopic procedures. The presenting case involved an inpatient with a complex medical history and a DNR order in place. The patient had a significant upper-GI bleed and required emergency endoscopy. Because the patient was incapable of consenting, the physician contacted the surrogate decision-maker (SDM), who consented to the procedure. The physician did not revisit the DNR order, assuming it would automatically apply during endoscopy. Unfortunately, the patient became apneic and had a pulseless arrest in the endoscopy suite; the DNR order was respected and the patient died. This case drew our attention to the fact that cardiopulmonary events requiring CPR may occur during endoscopy, yet there is a lack of guidance from professional bodies that guide gastroenterology practice on the management of DNR orders when endoscopy or other non-surgical procedures are considered.
The lack of such guidance around the management of pre-existing DNR orders is problematic as there is the potential for undesirable clinical outcomes. We proposed a model aimed at augmenting patient autonomy and protecting clinicians from liability concerns.
The management of existing DNR orders has been extensively discussed in the context of surgery and anesthesia. Professional bodies in anesthesia across jurisdictions have guidelines which mandate clinicians to revisit DNR orders prior to surgery. While surgery and endoscopy are different in terms of the degree of invasiveness, recommendations for the perioperative period are applicable to the ‘peri-endoscopic’ period.
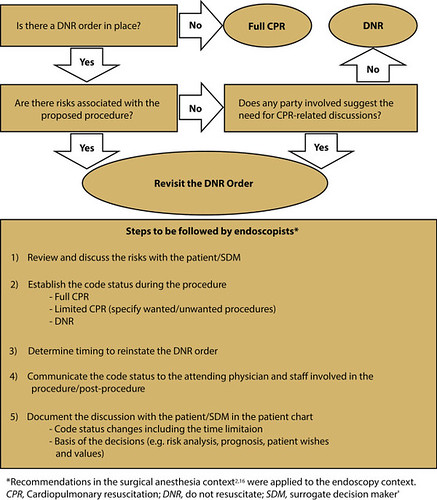
We have formulated a model for managing DNR orders in non-surgical contexts by drawing on guidelines/best practices for anesthesiologists. Our model suggests that DNR orders should be revisited based on anticipated risks of the procedure and any CPR-related concerns expressed by the patient/SDM or staff should a life-threatening event occur during the proposed procedure. The DNR/CPR discussion may be routinely integrated in the consent process by clarifying the risks of cardiovascular complications involved in the procedures including sedation, or the underlying conditions that may render the patient vulnerable. Depending on the outcome of the DNR/CPR conversation, the code status can remain the same or be modified for a specified time frame around the procedure. Specific circumstances such as when to reinstate the DNR order (if suspended) or events due to iatrogenic causes must also be addressed.
Finally, we suggest professional bodies in non-surgical disciplines consider drafting guidelines on revisiting DNR orders to maximize patient autonomy and to minimize staff concerns.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.

Thhanks for this blog post