
Post written by Jose Ignacio Vargas, MD, from the Gastroenterology Department and School of Medicine, Pontificia Universidad Católica de Chile, and the Endoscopy Unit, Hospital Clínico Universidad Católica de Chile, Santiago, Chile.
The focus of our study was to assess the effectiveness of the ingestion of different cleaning solutions before upper gastrointestinal in the evaluation and visibility of gastric mucosa endoscopy in a double-blinded, randomized, controlled trial.
The detection of gastric lesions through a complete evaluation of gastric mucosa is a major objective in upper endoscopy. It has been estimated that approximately 10% of gastric cancers were missed on previous endoscopic examinations, and poor visibility because of mucus covering the mucosa is one of the potential factors involved. The use of cleaning agents as preparation for upper gastrointestinal endoscopy is not the standard in western countries. Several studies have reported that the ingestion of cleaning agents before upper endoscopy could improve the visibility of gastric mucosa and, presumably, improve lesion detection. However, the negative comparator in all of these studies was the use of water alone before procedure compared to active cleaning agents, and none have evaluated only fasting as a control group, the most common condition in our centers. To that extent, the usefulness of the ingestion of cleaning agents before the procedure, such as Simethicone and N-acetylcisteine, has been conflicting. Therefore, comparing these cleaning agents alone or in combination to fasting and to the use of water through a randomized controlled trial was desirable. Moreover, Pronase has been the agent used in most of the studies, but it is not available in many countries outside of East Asia. Consequently, we used and tested a widely available mucolytic agent in our study (N-acetylcisteine).
Our results showed that the use before upper endoscopy of Simethicone plus N-acetylcisteine was superior to fasting and to the use of water alone in achieving an adequate visibility of gastric mucosa in different segments of the stomach, suggesting also a dose-dependent effect for N-acetylcisteine. Water alone had the worse score of all the groups in the gastric visibility score, and it’s use should possibly be discouraged. Also, we found that the use of Simethicone alone was not superior to fasting or water, a finding that could be useful in recommending adding N-acetylcisteine in centers where the use of Simethicone before endoscopy is instituted. Although the design of the study was not conceived to find a difference in lesion detection, the use of Simethicone plus N-acetylcisteine did provide a higher proportion of positive findings during upper endoscopy, suggesting that the ingestion of solutions containing these agents before the procedure could lead to a higher yield in detecting clinically significant lesions. However, this needs to be directly assessed in futures studies.
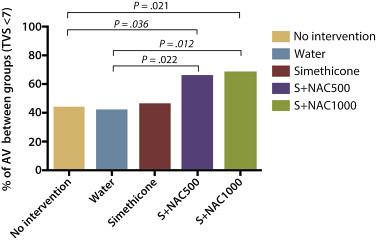
Figure 3. Percentage of adequate visibility (AV) for the study groups.
Our study also highlights the need for a standardized and validated scale for evaluating the visibility and cleaning of gastric mucosa during upper endoscopy, similar to the ones existing to evaluate the adequacy of preparation for colonoscopy (ie, Boston bowel preparation scale).
Considering the results of our study and current available evidence, we think that quality recommendations should move forward in the next years to advise the use of cleaning solutions before upper endoscopy to maximize the diagnostic yield of the procedure.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
