
 Post written by Wai K. Leung, MD, from the Department of Medicine, University of Hong Kong, Hong Kong, China.
Post written by Wai K. Leung, MD, from the Department of Medicine, University of Hong Kong, Hong Kong, China.
Gastric cancer is still the fifth most common cancer in the world with approximately one million new patients being diagnosed each year. Although upper endoscopy remains the gold standard for diagnosis of gastric cancer and pre-neoplastic gastric lesions, how often it should be performed or repeated remains uncertain. Unlike colonoscopy and colorectal cancer, there is no data to support that upper endoscopy could alter the prognosis of patients with gastric cancer.
We aimed to determine the association between intervals of prior upper endoscopy and the mortality of gastric cancer patients by using the Taiwan’s National Health Insurance Research Database.
We identified 20,066 newly diagnosed gastric cancer patients between 2002 and 2007. After excluding gastroscopy performed within 6 months of cancer diagnosis and matching for baseline discrepancies, cancer patients were divided into 3 groups according to intervals of prior gastroscopy (<2 years, 2-5 years, and >5 years). We found that when compared to the >5Y cohort, the hazard ratio of all-cause mortality for the <2Y and 2-5Y cohorts was 0.80 (95% CI, 0.72-0.89; P<0.001) and 0.83 (95% CI, 0.76-0.91; P<0.001), respectively. The HRs of gastric cancer-specific mortality was also significantly lower in the <2Y (0.80; 95% CI, 0.71-0.91; P<0.001) and 2-5Y cohorts (0.83; 95% CI, 0.75-0.93; P<0.001). In conclusion, we found that gastric cancer patients who had gastroscopy performed within 5 years prior to cancer diagnosis have significantly lower all-cause as well as cancer-specific mortality.
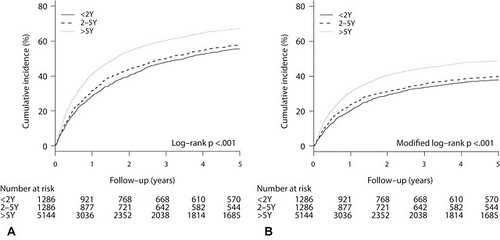
Figure 2. Cumulative incidences of all-cause mortality and gastric cancer–specific mortality in patients with gastric cancer who had prior gastroscopy at different time intervals. A, All-cause mortality. B, Gastric-cancer–specific mortality. Calculation and comparison of cumulative mortalities were conducted by using the Kaplan-Meier method (P < .001 for both all-cause and gastric cancer–specific mortalities when comparing <2 Y versus >5 Y and 2 to 5 Y versus >5 Y cohorts. P value was not significant when we compared <2 Y versus 2 to 5 Y cohorts).
Our results may support the role of more frequent endoscopic examinations in patients at high risk of gastric cancer.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
