
Post written by Eiichiro Yamamoto, MD, PhD, Yoshihito Tanaka, MD, and Hiromu Suzuki, MD, PhD, from the Department of Molecular Biology, Sapporo Medical University School of Medicine, Sapporo, Japan, and the Department of Digestive Disease Center, Akita Red Cross Hospital, Akita, Japan.
Sessile serrated adenoma/polyps (SSA/Ps), which are precursor lesions of colorectal cancer (CRC) with BRAF mutation and the CpG island methylator phenotype (CIMP), and SSA/Ps with cytological dysplasia (CD) are at high risk for developing CRC. The aim of this study was to clarify the endoscopic and molecular signatures of SSA/Ps, with and without CD.
Detection and removal of precancerous lesions is essential to prevent CRCs. High-resolution magnifying colonoscopy is a powerful diagnostic tool for observing the microsurface structure (pit patterns) of lesions, which enables detection of conventional adenomas with malignant potential. SSA/Ps with CD are well known as premalignant lesions which are at high risk of developing CRC. We have experienced some cases of SSA/P with CD, which rapidly progressed to carcinoma. We believe that accurate colonoscopic diagnosis of SSA/Ps with CD would contribute to CRC prevention.
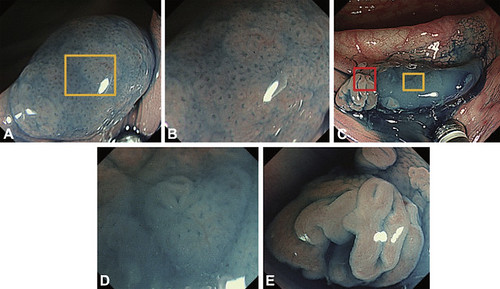
Figure 1. Colonoscopic views of representative serrated lesions. A, Colonoscopic view of a representative sessile serrated adenoma/polyp (SSA/P) showing a Type II-O pit pattern. B, Magnified view of the SSA/P indicated by the yellow box in A. C, Colonoscopic view of a representative SSA/P with cytologic dysplasia showing a Type II-O plus IV pit pattern. D, Magnified view of the SSA/P portion indicated by the yellow box in C. E, Magnified view of the cytologic dysplasia portion indicated by the red box in C.
In the previous study, we have reported a novel surface microstructure Type II-Open pit pattern (Type II-O), which is highly specific to SSA/P with BRAF mutation and CpG island methylator phenotype (CIMP). In order to consolidate the usefulness of the pit pattern to detect SSA/Ps at high risk of malignant progression, we focused on SSA/Ps with CD in this study. Integrative analysis of endoscopic, pathological, and molecular features in a cohort of serrated lesions clearly demonstrated that Type II-O plus adenomatous pit patterns (Type III or IV) are common features of SSA/Ps with CD in both the proximal and distal colon.
Furthermore, we also determined whether the extent of the adenomatous pit patterns was associated with the clinicopathological or molecular features of SSA/Ps with CD. We found that 4 tumors with the least Type III/IV area (less than 10%) exhibited MLH1 methylation, which could drive malignant progression through inducing microsatellite instability. These results indicate that, not the extent of the Type III/IV areas, but the coexistence of adenomatous pit patterns is the hallmark of cancer risk in SSA/Ps.
In summary, our results suggest that the Type II-O plus III/IV pit pattern is a hallmark of serrated lesions at high risk of developing CRCs, irrespective of the extent of the Type III/IV portion. Our results should be validated in a multi-center prospective study with a larger population. Also, discrimination between SSA/Ps and traditional serrated adenomas (TSAs) remains another issue to be addressed in a future study.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
