


Post written by Navin L. Kumar, MD and John R. Saltzman, MD, from the Brigham and Women’s Hospital, Division of Gastroenterology, Hepatology and Endoscopy, and Harvard Medical School, Boston, Massachusetts.
The focus of our study was to assess whether an increase in blood urea nitrogen (BUN) at 24 hours of presentation is predictive of worse clinical outcomes in acute nonvariceal upper GI bleeding (UGIB).
Current guidelines advise that all patients with acute nonvariceal UGIB undergo risk stratification based on validated prognostic scores. However, available scoring systems require multiple inputs of data, and accordingly, a recent study showed that only 30% of physicians use a risk stratification score when evaluating a patient with UGIB. Thus, a need exists to identify a solitary predictor of outcomes in UGIB that is easily calculated by providers.
In acute pancreatitis, a rise in BUN at 24 hours of presentation was shown to be a strong predictor of mortality. We hypothesized that an increase in BUN would also predict worse outcomes in the similarly resuscitation-requiring condition of acute nonvariceal UGIB.
We conducted a retrospective cohort study at a single academic center of patients admitted with nonvariceal UGIB. We defined an increase in BUN as a rise in BUN at 24 hours of hospitalization compared with the BUN at presentation. Our primary outcome was a composite of inpatient death, inpatient rebleeding, need for surgical or interventional radiologic intervention, or endoscopic re-intervention.
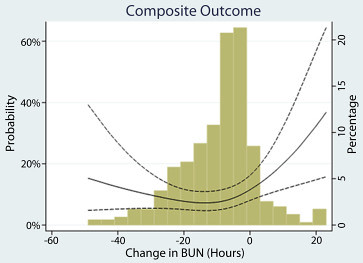
Figure 1. Test for nonlinear relationship between change in blood urea nitrogen (BUN) and the composite outcome.
In our study of 357 patients, we found that patients with an increase in BUN were more likely to experience the composite outcome compared with patients who had a decreased or unchanged BUN at 24 hours (22% vs. 9%, P=0.014). Patients with a rise in BUN also had a higher risk of inpatient death than those with a decreased or unchanged BUN (8% vs. 1%, P=0.004). In a logistic regression model that adjusted for the AIMS65 score, an increase in BUN remained an independent predictor of the composite outcome (OR = 2.75; P=0.026).
Restoration of intravascular volume is a critical step in the early management of acute nonvariceal UGIB. We suspect that a rise in BUN at 24 hours of hospitalization identifies those patients who were under-resuscitated, thereby leading to worse outcomes. Prospective studies are needed to further explore this association and identify optimal treatment strategies for those patients found to have a rising BUN at 24 hours.
In summary, we found that a rise in BUN at 24 hours is a significant and solitary predictor of worse outcomes in acute nonvariceal UGIB. The increase in BUN at 24 hours is likely a marker for under-resuscitation and highlights the importance of adequate volume resuscitation in optimally managing patients with upper GI bleeding.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
