
Post written by Michael Kevin Dougherty, MD, from the University of North Carolina Division of Gastroenterology and Hepatology.
The purpose of this study was to estimate the rate of perforations and other adverse events related to elective endoscopic esophageal dilation in patients with eosinophilic esophagitis (EoE).
Many patients with EoE struggle with significant dysphagia and food impactions due to fibrosis that may respond slowly—or sometimes not at all—to medical and dietary therapy. Dilation provides the opportunity for more rapid symptomatic relief as well as prevention of the morbidity of food impaction. Due to early reports of increased risk of perforation in EoE, however, there has been a reluctance to position this useful therapy toward the front of management algorithms for the condition. We suspected that the magnitude of this risk may be overestimated in the minds of practitioners, compared to what is supported by the published literature.
Random effects meta-analysis revealed a perforation rate of 0.033% (95% CI, 0-0.225%) per procedure. Even the upper limit of this confidence interval is no higher than rates that are generally quoted for dilation of all benign esophageal strictures (less than 0.4%). None of the 9 perforations identified required surgical intervention or resulted in mortality. Further, we identified several new studies that suggested dilation can also be performed safely in pediatric patients, with no signal of a difference between bougie and through-the-scope balloon dilators. The literature comprised largely uncontrolled, observational studies, so there is still a need for good quality research to increase confidence in the precision of the estimate. When done carefully and methodically, however, it is unlikely that elective dilation in EoE contributes excessive risk to the patient. Increased confidence in the safety of this procedure should pave the way for incorporation into future experimental studies that refine dilation’s place within the greater scheme of care for the EoE patient, as well as increase access of a potentially dramatic symptom-relieving intervention for EoE patients in the community.
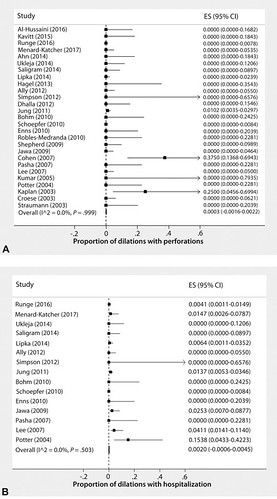
Figure 2. Forest plots of random-effects meta-analysis for (A) perforation, (B) hospitalization, (C) clinically significant chest pain, and (D) unspecified chest pain. Case series and case reports not displayed. The boxes represent the point estimate, and the bars represent the 95% confidence intervals that are left-truncated because it is not possible to have a proportion less than zero in this meta-analysis. I2 is the percentage of total variation across studies because of heterogeneity rather than chance. ES, Effect size; CI, confidence interval.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
