
Post written by Parit Mekaroonkamol, MD, Sunil Dacha, MD, and Qiang Cai, MD, PhD, from Emory University School of Medicine.

Gastric per-oral endoscopic pyloromyotomy (GPOEM) is an emerging endoscopic procedure for treatment of gastroparesis. Due to its novelty, the existing data on its safety and efficacy is lacking. The purpose of our study was to systematically assess the clinical responses and improvement in quality of life after GPOEM in patients with medically refractory gastroparesis using standardized clinical monitoring tools, ie, gastroparesis cardinal symptoms index (GCSI) score and short-form 36 (SF36) questionnaire, in addition to gastric emptying scintigraphy (GES) over a 12-month follow-up period.
Gastroparesis is a chronic debilitating disease with a complex pathophysiology, rendering inconsistent and often ineffective responses to available treatments. With very limited therapeutic options, GPOEM has an exciting potential to become the forefront of gastroparesis treatment.
Our study showed an overall clinical success rate of 81% with remarkable improvement across all outcomes, including GES, GCSI, and SF36 scores. These favorable responses appeared to have sustained throughout the 12-month follow-up period, with 87% of patients able to maintain or gain body weight. This is the first report of improvement in quality of life in patients with medically refractory gastroparesis following GPOEM. There were no major adverse events associated with the procedure. Interestingly, subgroup analyses demonstrated improvement in nausea, vomiting, and early satiety but not in bloating or pain. These findings were in line with prior studies that suggested better response of pylorus-directed intervention in patients with predominant nausea/vomiting. The reasons for the varying degree of responsiveness remain unclear. Etiology of gastroparesis has been reported to affect outcomes of gastroparesis treatment, but this was not significantly observed in our study, even though all 3 patients who failed GPOEM had diabetic gastroparesis. Currently, there are no reliable ways to predict which patients would respond to GPOEM. We hypothesized that patients with pylorospasm would have a high likelihood of responding to pyloromyotomy; however, optimal tools to identify these patients such as measurement of pyloric distensibility, transpyloric pressure, and distally retained radiolabeled are not readily available. This perhaps should be the focus of future research. Even though our study was limited by its retrospective nature and small sample size, our results underscore the efficacy of GPOEM as an incision-free, minimally-invasive method for endoscopic pyloroplasty, proving it a viable option for refractory gastroparesis.
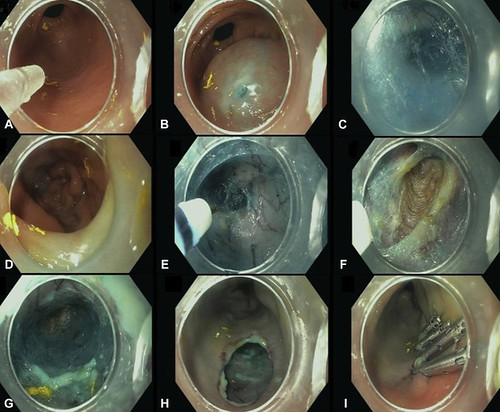
Figure 1. GPOEM procedure steps. A, Gastric antrum; B, mucosal bleb; C, submucosal tunnel; D, bluish color in duodenal bulb to confirm tunnel depth; E, pyloric ring; F, pyloromyotomy; G, submucosal tunnel; H, mucosotomy site; I, mucosotomy closure with clips.
Since GPOEM is a new endoscopic therapeutic modality for gastroparesis, the long-term outcome is unknown at this time.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
