
Post written by David J. Tate, MA (Cantab), MBBS, MRCP, from Westmead Hospital, Department of Gastroenterology and Hepatology, and Westmead Campus, University of Sydney Medical School, Sydney, Australia.
Recurrence is the main limitation of wide-field endoscopic mucosal resection (EMR) for large laterally spreading colonic lesions (LSL). We aimed to derive a set of clinically useful parameters that might predict the likelihood that a given lesion would recur.
Adenoma recurrence after endoscopic mucosal resection imposes medicolegal obligations, healthcare costs, and patient inconvenience. A better understanding of the temporal behavior of recurrence after EMR and how to predict whether it will occur may improve clinical outcomes.
In this study, we have been able to accurately stratify the risk of adenoma recurrence after piecemeal EMR using a simple 4-point clinical score (the Sydney EMR Recurrence Tool, SERT). Identified independent predictors of residual or recurrent adenoma that made up SERT were size of lesion ≥ 40mm (OR 2.47), intra-procedural bleeding requiring endoscopic control (OR 1.78), and high-grade dysplasia (OR 1.72) in the resection specimen. The score was derived from a random half of a prospective multi-center cohort of more than 2000 patients over 8 years and validated on the remainder.
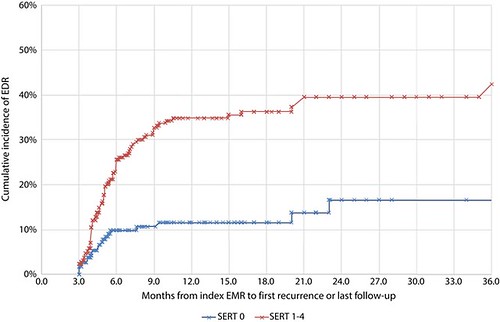
Figure 5. Kaplan-Meier plot of endoscopically determined recurrence (EDR) as stratified by the presence (Sydney EMR recurrence tool score [SERT] 1-4) or absence (SERT = 0) of high-risk features for recurrence at the initial EMR. Lesions displayed are from the validation cohort (n = 589). Log-rank test; P < .001. EDR, endoscopically determined recurrence; SERT, Sydney EMR recurrence tool.
SERT=0 lesions had significantly less cumulative incidence of RRA over time: 9.8%, 11.6%, 11.6%, and 16.6% cumulative incidence of EDR at 6, 12, 18, and 36 months, respectively. SERT 1-4 lesions had 23.0%, 34.9%, 36.3%, and 39.5% cumulative incidence over the same intervals.
Our study represents a step forward in the understanding of the temporal behavior of adenoma recurrence after EMR of large LSL, and we believe it will be of substantial interest to readers of Gastrointestinal Endoscopy. We have shown that adenoma recurrence after piecemeal resection of large colonic LSL is predictable in its time course and stratifiable by a simple clinical score, allowing EMR practitioners to reliably predict which lesions will recur and triage these to earlier and more rigorous follow-up. Given that endoscopic treatment of recurrence is successful in the vast majority of cases, we believe this knowledge will further affirm the cost effectiveness, safety, and efficacy of EMR in the treatment of large colonic LSLs versus other treatment options.
To this end, we have suggested that low-risk lesions (SERT=0, 40% of our cohort) may be safely surveyed at 18 months post EMR because the cumulative incidence of recurrence is low (11.6%) and does not appreciate greatly to this point from the standard surveillance interval of 6 months (9.8%). This approach effectively skips the first surveillance procedure for low-risk lesions and may lead to cost savings for healthcare systems and avoidance of unnecessary colonoscopy for patients. We have emphasized the need for close attention to removal of synchronous advanced adenomas at the referral and EMR procedures if this approach is to be successful.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
