
 Post written by Yasuki Hori, MD, PhD, from the Department of Gastroenterology and Metabolism, Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan.
Post written by Yasuki Hori, MD, PhD, from the Department of Gastroenterology and Metabolism, Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan.
We focused on predictors for solid food intake after self-expandable metal stent (SEMS) placement for malignant gastric outlet obstruction, not only patient-related factors but also stent-related factors. We consider the identification of stent-related factors for poor oral intake to be important because it can be prevented by changing stent types.
No clinical difference, apart from stent migration, was observed between patients with uncovered and covered SEMSs. On the basis of stent expansion rate, under expansion on the procedure day causes early tumor ingrowth in uncovered SEMS, which may be resolved using covered SEMS. GI obstruction caused by anastomotic sites or metastatic cancer may be an indication for covered SEMS by the higher incidence of insufficient stent expansion.
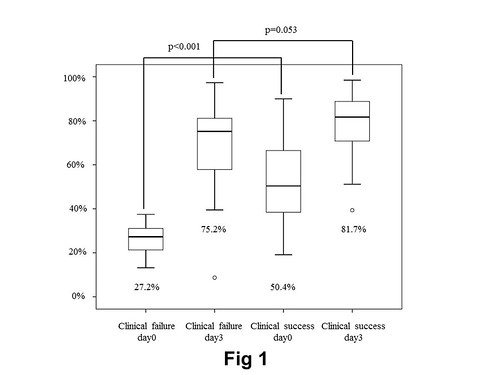
Comparison of GOO score improvement and stent expansion
on days 0 and 3 in the U-SEMS group. The stent expansion rate on day
0 was significantly higher in the improvement subgroup than in the
poor improvement subgroup (50.4% vs 27.2%; P < .001). No significant
difference between the improvement and poor improvement subgroups
was observed on day 3 (81.7% vs 75.2%; P Z .053). GOO, gastric outlet
obstruction; U-SEMS, uncovered self-expandable metal stent.
If only uncovered SEMS is available, clinicians should pay more attention to the SEMS under expansion on the procedure day.

Comparison of GOO score improvement and stent expansion
on days 0 and 3 in the C-SEMS group. The stent expansion rate did not
affect GOO score improvement (day 0: 53.1% vs 49.5%, P Z .365; day
3: 90.0% vs 91.2%, P Z .452). GOO, gastric outlet obstruction; C-SEMS,
covered self-expandable metal stent.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
