
 Tadahisa Inoue, MD, from the Department of Gastroenterology, Gifu Prefectural Tajimi Hospital, in Gifu, Japan, describes this New Methods article “Feasibility of the placement of a novel 6-mm diameter threaded fully covered self-expandable metal stent for malignant hilar biliary obstructions (with videos).”
Tadahisa Inoue, MD, from the Department of Gastroenterology, Gifu Prefectural Tajimi Hospital, in Gifu, Japan, describes this New Methods article “Feasibility of the placement of a novel 6-mm diameter threaded fully covered self-expandable metal stent for malignant hilar biliary obstructions (with videos).”
The focus of this study was to evaluate the safety and efficacy of the placement of a novel 6-mm threaded fully covered self-expandable metal stent (T-FCSEMS) for unresectable malignant hilar biliary obstruction (MHBO).
Biliary stents placed in patients with unresectable tumors will ideally remain patent without adverse events until death. However, progress in chemotherapy, including the treatment of cholangiocarcinomas and gallbladder carcinomas, is expected to prolong the prognoses of patients with MHBO. For this reason, the frequency of recurrent biliary obstruction (RBO) increases even when placing an uncovered self-expandable metal stent (USEMS), and reintervention is required. However, preventing tumor ingrowth can be difficult for the USEMS, and it can never be removed; thus, reintervention for RBO is often troublesome.
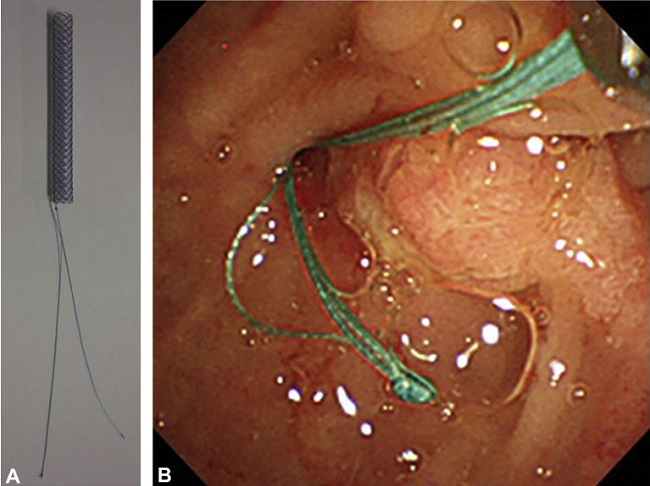
Figure 1. The novel 6-mm threaded fully covered self-expandable metal stent (TaeWoong Medical Co, Ltd, Seoul, Korea). A, The thread is tied to the duodenal side of the stent. B, The threads are drawn from the duodenal papilla into the duodenum.
The availability of T-FCSEMS may solve these issues. This novel stent prevents tumor ingrowth, and stent replacement can be performed at the time of reintervention after the stent has been removed using the thread. Thus, performing the reintervention.
The result of this study determined that T-FCSEMS placement for MHBO was associated with a high technical success rate, and the time to RBO was favorable. In addition, T-FCSEMS removal was successful in all patients in whom it was attempted during reinterventions for RBO, and the success rate was 100% for endoscopic reintervention. However, liver abscesses developed because of posterior bile duct occlusions in the posterior segments 8 and 22 days after T-FCSEMS placement in 2 cases whose stents were placed across the posterior bifurcation.
T-FCSEMS placement is a promising option for MHBO, particularly in patients with a high probability for reintervention, and the stents do not reach the intrahepatic bile duct bifurcation. However, the indications for the use of this stent should be carefully considered in patients who require placement across the intrahepatic bile duct bifurcation, such as those categorized as Bismuth types III and IV, because intrahepatic bile duct occlusion can occur.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
