
 Joo Ha Hwang, MD, PhD, from the Harborview Medical Center, University of Washington, in Seattle, Washington, USA reports on this Review article, “Screening and surveillance for gastric cancer in the United States: Is it needed?”
Joo Ha Hwang, MD, PhD, from the Harborview Medical Center, University of Washington, in Seattle, Washington, USA reports on this Review article, “Screening and surveillance for gastric cancer in the United States: Is it needed?”
This is a review article that examines the published data on risk factors for gastric cancer and methods for gastric cancer screening. We felt that this review was necessary to increase awareness of the significance and incidence of gastric cancer in the United States.
The perception of gastric cancer in the US is that it is a relatively uncommon disease and that screening for gastric cancer is not needed. However, most people do not realize that gastric cancer is more common than esophageal cancer in the US. We have clear guidelines on screening for Barrett’s esophagus and esophageal cancer; however, no clear guidelines exist for screening for gastric cancer even though there are populations in the United States that are at high risk for developing gastric cancer, particularly immigrants from East Asia, Russia, and parts of South America. There also seems to be uncertainty in the significance of gastric intestinal metaplasia (GIM) and whether GIM requires surveillance. The aim of this review was to identify risk factors for gastric cancer, evaluate screening methods, and propose an algorithm for gastric cancer screening in the US.
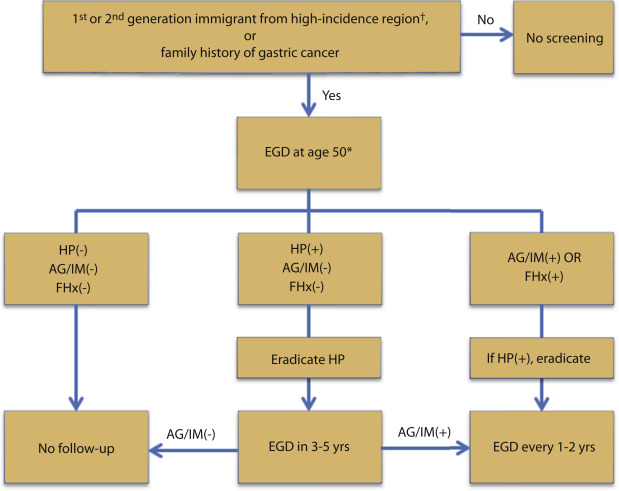 Figure 3. Suggested screening algorithm for gastric cancer in the United States. †East Asia, Russia, and South America. *If there is a first-degree relative with gastric cancer, start screening 10 years before the age at diagnosis in the first-degree relative or age 50 (whichever is earlier). HP, H pylori; FHx, family history of gastric cancer; AG, atrophic gastritis; IM, intestinal metaplasia.
Figure 3. Suggested screening algorithm for gastric cancer in the United States. †East Asia, Russia, and South America. *If there is a first-degree relative with gastric cancer, start screening 10 years before the age at diagnosis in the first-degree relative or age 50 (whichever is earlier). HP, H pylori; FHx, family history of gastric cancer; AG, atrophic gastritis; IM, intestinal metaplasia.
This review identified several reports demonstrating that particular ethnic populations that have a significantly higher incidence of gastric cancer than the general population in the US, especially immigrants from Korea and Japan. Furthermore, intestinal metaplasia is reported to have a relative risk of 6.4 (95% CI: 2.6-16.1) for progressing to gastric cancer. In addition, family history of gastric cancer was also considered to be a significant risk factor. Based on this review, we propose an algorithm to consider for gastric cancer screening and surveillance of GIM in the US (see figure).
There is also an increasing interest in the GI community in performing endoscopic submucosal dissection (ESD); however, the opportunity (number of cases where it is indicated) is limited. The ideal application of ESD is for the treatment of high-grade dysplasia and early gastric cancer. In order to identify these lesions, some form of screening for gastric cancer is necessary. If screening for gastric cancer were implemented, it is likely that substantially more lesions amenable to ESD would be identified.
Read the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
