
 Federico Iacopini, MD, from Gastroenterology and Digestive Endoscopy, Ospedale San Giuseppe, in Rome, Italy discusses this Original Article “Prognostic variables for the clinical success of flexible endoscopic septotomy of Zenker’s diverticulum.”
Federico Iacopini, MD, from Gastroenterology and Digestive Endoscopy, Ospedale San Giuseppe, in Rome, Italy discusses this Original Article “Prognostic variables for the clinical success of flexible endoscopic septotomy of Zenker’s diverticulum.”
Flexible endoscopic septotomy for Zenker’s diverticulum has a large popularity due to its mini-invasiveness compared to endostapling and surgery but strong long-term clinical data on its efficacy lack, and most studies evaluated only dysphagia among all related symptoms (regurgitation, cough, aspiration). Finally, the technique for flexible endoscopic septotomy is not yet standardized.
This study evaluates the asymptomatic rates of flexible endoscopic septotomy for Zenker’s diverticulum defined as the almost complete ablation of all related symptoms in a large population followed for at least 24 months after treatment. Moreover, it identifies for the first time the prognostic variables of success, indispensable to define the role of flexible endoscopy in the therapeutic algorithm. 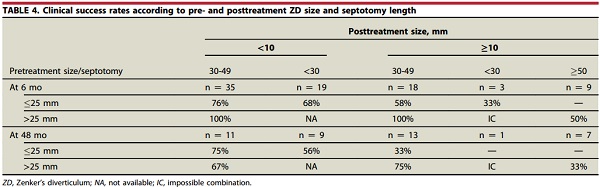 The overall clinical efficacy of flexible endoscopic septotomy of Zenker’s diverticulum is lower than previously reported. However, the combination of Zenker’s size and length of septotomy safely achievable by flexible endoscopy identifies 3 groups of patients with different prognosis, the best being those with a 30-50 mm Zenker’s in which septotomy is >25 mm.
The overall clinical efficacy of flexible endoscopic septotomy of Zenker’s diverticulum is lower than previously reported. However, the combination of Zenker’s size and length of septotomy safely achievable by flexible endoscopy identifies 3 groups of patients with different prognosis, the best being those with a 30-50 mm Zenker’s in which septotomy is >25 mm.
Flexible endoscopic septotomy is the best approach for Zenker’s diverticulum comprised between 30 and 50 mm and highly effective in a single session. On the contrary, a flexible endoscopic retreatment is required for small and large diverticula due to an incomplete septotomy or to ablate a residual pouch in those <30 mm and >50 mm, respectively. Surgery and endostapling may be good alternatives in these last cases.
Find the abstract for this article here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.

Dear Dr. Iacopini. Congratulations to you and your group for this nice paper. You clearly demonstrated that the size of the diverticulum and the extension of the endoscopic septotomy can predict clinical success. How did you measure those variables? Endoscopically, radiologically, both? Thank you.
Dear Dr Fauze, Thank you for your comment. The Zenker’s size (depth) has been measured before and after septotomy at endoscopy using a catheter with homemade markings every 5 mm on its length. The tip of the cateter was gently put at the bottom of the divertulum.
Dear Dr Fauze,
thank you very much for your comment.
The Zenker’s size/depth was measured endoscopically before and after septotomy using a catheter with homemade markings every 5 mm. The length of septotomy was measured as the difference between preoperative and postoperative size/depth of the Zenker’s diverticulum.
Thank you again.