
 Do Hyun Park, MD, PhD, from the Division of Gastroenterology, Department of Internal Medicine, University of Ulsan College of Medicine, Asan Medical Center, in Seoul, Korea shares this Original Article “Feasibility and safety of a fully covered self-expandable metal stent with antimigration properties for EUS-guided pancreatic duct drainage: early and midterm outcomes (with video).”
Do Hyun Park, MD, PhD, from the Division of Gastroenterology, Department of Internal Medicine, University of Ulsan College of Medicine, Asan Medical Center, in Seoul, Korea shares this Original Article “Feasibility and safety of a fully covered self-expandable metal stent with antimigration properties for EUS-guided pancreatic duct drainage: early and midterm outcomes (with video).”
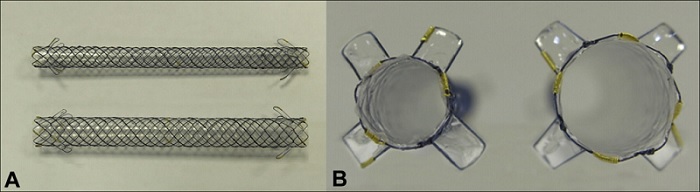
The focus of this study was to evaluate the feasibility and safety of a fully covered self-expandable metal stent (FCSEMS) with antimigration properties for EUS-guided pancreatic duct drainage (EUS-PD) in patients with painful obstructive pancreatitis.
EUS-PD has been used for painful obstructive pancreatitis after failed endoscopic retrograde pancreatography (ERP). Until now, EUS-PD with transmural plastic stenting has usually underwent. However, stent-related adverse events such as stent migration, failures in stent placement, or pancreatic fluid leakages have been of concern in transmural plastic stenting procedures. EUS-guided transmural drainage with a fully covered self-expandable metal stent (FCSEMS) has been increasingly used for biliary, gallbladder, and pseudocyst drainage because of its simplified placement method, shortened procedure time, potential reduction of adverse events, and prolonged stent patency. To date, however, little is known about the role of EUS-PD with transmural metal stenting. This study was important because of the first report on EUS-PD with an FCSEMS for painful obstructive pancreatitis.
In our study, EUS-PD with an FCSEMS was technically feasible and relatively safe for patients with painful obstructive pancreatitis after failed ERP. EUS-PD was successful in all 25 patients (technical success, and clinical success was 100%). Pain score also improved after FCSEMS placement. No stent related adverse events such as stent migration, stent clogging, pancreatic sepsis, and pancreartic ductal stricture was observed. In permanent stenting group (n=13), 11 patients had malignant main pancreatic duct obstruction. These patients did not show stent malfunction during follow-up periods. An FCSEMS placement may minimize stent exchange, potentially without exchange, as compared with plastic stent placement for patients who are expected to survive for longer than 4 to 6 months. There are not many published articles about the use of pancreatic stents in malignant symptomatic pancreatic duct obstruction so this could be another useful information from our study.
Because this study has only the early and mid-term outcomes, long-term outcomes on EUS-PD with an FCSEMS may be required in a further study. Moreover, a randomized trial comparing EUS-PD with long-term FCSEMS and plastic stents with painful obstructive pancreatitis after ERP may be warranted.

Congratulations to the authors for the nice job. Should the obstruction of side branches be of concern with the use of fully covered metallic stents in the main pancreatic duct?
Thank you for your excellent comment. We selected stents with 6- or 8-mm diameters, which is according to the diameter of the dilated pancreatic duct. This may optimize the radial force of an FCSEMS (fully covered self expandable metal stent), thereby preventing further compression of the covering membrane and wire mesh to the MPD. Covering membrane was placed inside of wire mesh in this FCSEMS. Therefore, the flow of pancreatic fluid between the MPD and the covering membrane of FCSEMSs may be presumably allowed by low radial force (than 10-mm diameter) and stent design as the wick effect. This may explain that the obstruction of side branches may be minimal in the use of FCSEMS in the main pancreatic duct in this study.
I really enjoy reading your article. Thank you for posting this. Keep it up. God Bless.