
 Takuji Gotoda, MD, PhD, FASGE, from the Department of Gastroenterology and Hepatology, Tokyo Medical University, in Tokyo, Japan discusses this Original Article “Usefulness of a traction method using dental floss and a hemoclip for gastric endoscopic submucosal dissection: a propensity score matching analysis (with videos).”
Takuji Gotoda, MD, PhD, FASGE, from the Department of Gastroenterology and Hepatology, Tokyo Medical University, in Tokyo, Japan discusses this Original Article “Usefulness of a traction method using dental floss and a hemoclip for gastric endoscopic submucosal dissection: a propensity score matching analysis (with videos).”
Endoscopic submucosal dissection (ESD) represents a significant advancement in therapeutic endoscopy resulting in complete local control. However, the technique of ESD is complicated and requires considerable expertise and a prolonged operation time. Especially, bleeding during submucosal dissection is often interfering endoscopic manipulation under good visualization. Poor visualization resulting from no traction renders the technique difficult, time-consuming, and prone to adverse events. In our exploratory study, we aimed to evaluate the efficacy of a simple traction method, which uses dental floss and a hemoclip and was developed to overcome the technical difficulties of ESD. It is well known that randomized controlled trials should be considered to be the most reliable form of evaluating scientific evidence. However, we should also consider that such studies have several drawbacks when examining techniques or procedures, such as the disadvantage of control patients in that they do not receive an effective technique or procedure. Then, we applied propensity score matching analysis in therapeutic endoscopy field.
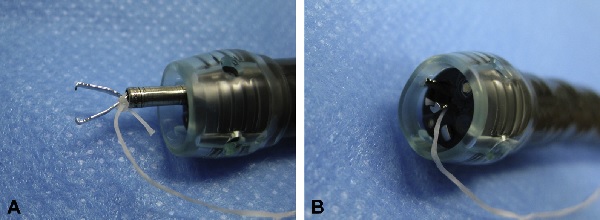 Figure 2. Preparation of the DFC. A, A long piece of dental floss is tied to the arm of the hemoclip. B, The hemoclip tied with dental floss is withdrawn into the transparent hood and the accessory channel of the endoscope to enable the insertion of the endoscope. DFC, traction method using dental floss and a hemoclip.
Figure 2. Preparation of the DFC. A, A long piece of dental floss is tied to the arm of the hemoclip. B, The hemoclip tied with dental floss is withdrawn into the transparent hood and the accessory channel of the endoscope to enable the insertion of the endoscope. DFC, traction method using dental floss and a hemoclip.
ESD with the traction method using dental floss and a hemoclip (DFC) was found to be significantly associated with a shorter procedure time, high curability, and safety. DFC method contributed to easier ESD procedures without compromising safety. To minimize sampling bias, propensity score matching analysis was employed between the ESD-DFC and conventional ESD groups using the above clinical factors.
The feasibility of a simple traction method using a hemoclip and long suture material, which was very similar to our concept has been already reported. However, dental floss may have additional advantages over silk sutures. The knot in the dental floss on the clip arm is tight and will not loosen, and only minimal mucosal injury may be caused due to pulley tension and contact with the dental floss, because the dental floss is shaped like a flat ribbon, in contrast to silk suture, which is thin and cylindrical in shape. Additionally, the preparation of the clip and the anchoring procedure were easy, and required only a few minutes. Furthermore, the procedure does not restrict endoscopic movement or limit the visual field because the hemoclip is small and the suture material is very thin.
DFC method facilitated rapid ESD through good visualization and appropriate traction of the submucosal layer, while ensuring high curability and safety. As this method has no critical disadvantage, it may be preferable to use this method as part of the standard procedure for ESD.
Find the abstract of this article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set fort

Dear Prof. Gotoda. Congratulations on your nice paper. Would you currently recommend the DFC method for all the cases of gastric ESD or exclusively for the challenging ones? Would you consider the presence of fibrosis a good indication for the DFC method? Thank you.
Dear Professor Maluf-Filho
Thank you for nice comments. Yes, I am recently doing all oesophageal, gastric and colorectal ESD uder DFC method. I believe that it is key to make nice visualization for safer and shorter ESD because the reason of uncontrollable bleeding is blinded condition. As for lesion with fibrosis, this method is also helpful o dissect fiber by fiber using needle type knives. However, I am always paying an attention whether muscle layer is lifted to much. Thus, the tension of DF should be carefully checked.
Thanks again, Takuji
Dear Prof. Gotoda,
Thank you so much for sharing such mindful concepts with us.
Fauze
Dear Professor Maluf-Filho
Thank you for your comments. Yes, I am doing recently all ESD under DFC method. I believe that it is key to make nice visualization during submucosal dissection because uncountable bleeding make ESD much difficult.
As for the lesion with submucosal fibrosis, it is of course helpful to dissect fiber by fiber. However, I am always paying attention whether muscle layer is lifting to much.
Thanks, Takuji