
 Gwang Ha Kim, MD from the Department of Internal Medicine at Pusan National University School of Medicine in Busan, Republic of Korea discusses his article “Factors associated with the outcomes of endoscopic submucosal dissection in pyloric neoplasms.”
Gwang Ha Kim, MD from the Department of Internal Medicine at Pusan National University School of Medicine in Busan, Republic of Korea discusses his article “Factors associated with the outcomes of endoscopic submucosal dissection in pyloric neoplasms.”
Endoscopic submucosal dissection (ESD) is a widely accepted treatment for premalignant lesions and early cancers in the stomach. However, in when a neoplasm is located at the pylorus, certain anatomical features of the pylorus adversely affect precise assessment of tumor margin and performance of ESD. Therefore, pyloric neoplasms are one of the most difficult lesions to resect with ESD.
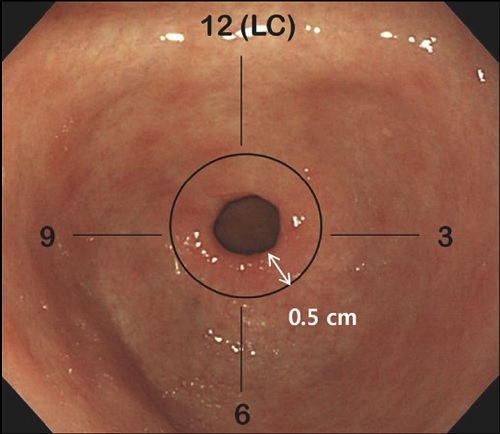 Figure 1. Endoscopic assessment of pyloric neoplasms. Pyloric neoplasms are defined as tumors with the distal margin located < .5 cm from the pyloric ring when the ring is fully opened. A clock-face orientation
Figure 1. Endoscopic assessment of pyloric neoplasms. Pyloric neoplasms are defined as tumors with the distal margin located < .5 cm from the pyloric ring when the ring is fully opened. A clock-face orientation
with the endoscope (with the lesser curve [LC] of the stomach in contiguity with the 12 o’clock of the pylorus) is used to classify directional distribution into 4 quadrants.
In this study, we tried to find the predictive factors for the incomplete resection in ESD for pyloric neoplasms. We classified pyloric tumors into pylorus only type (P-type) and pylorus-duodenal type (PD-type) according to their duodenal extension, and we also classified them into upper and lower hemispheric distribution after a clock-face orientation of the endoscope (with the lesser curve of the stomach in contiguity with the 12 o’clock of the pylorus).
As a whole, we showed a high rate for complete resection and a low rate of procedure-related complication for ESD of pyloric neoplasms. Complete resection rates differed significantly in relation to location (P-type vs PD-type, 79% vs 58%), directional distribution (upper hemisphere vs lower hemisphere of the pylorus, 67% vs 90%), tumor size (≤10 mm vs >10 mm, 84% vs 67%), and circumferential extent of pyloric mucosal resection (≤1/2 vs >1/2, 92% vs 62%). On multivariate analysis, tumor location (pylorus with duodenal extension; OR 5.747), hemispheric distribution (upper hemisphere; OR 4.906), and circumferential extent of resection (>1/2; OR 3.960) were independent factors associated with incomplete resection. These results provide important information to assist endoscopists, especially beginners and trainees, in assessing the difficulty of ESD of pyloric neoplasms before undertaking the procedure.
Read the abstract for this article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
