
Post written by Roberto de Sire, MD, PhD, from the Endoscopy Unit, Gastroenterology Department, Humanitas Research Hospital IRCCS, Rozzano, and the IBD Unit, Department of Clinical Medicine and Surgery, University Federico II, Naples, Italy.

Our study explored a timely and practical question in therapeutic endoscopy: among the newer endoscopic submucosal dissection (ESD) strategies developed for colorectal lesions, how do underwater ESD (UW-ESD) and traction-assisted ESD (T-ESD) compare? Both techniques were designed to address some of the most important limitations of conventional ESD, especially with technically demanding colorectal resections. By conducting a network meta-analysis of randomized controlled trials, we aimed to better define their relative performance in terms of efficacy and safety.
Colorectal ESD continues to evolve, and innovation is increasingly driven by techniques that make dissection safer, faster, and more reproducible. UW-ESD and T-ESD are among the most promising approaches, but until now the evidence has been fragmented, with no direct randomized comparison between them. We felt it was important to bring together the highest-quality available data to help clinicians move beyond anecdotal preference and toward a more evidence-based understanding of when and why these techniques may be useful.
Our findings show that UW-ESD and T-ESD are effective and safe strategies for colorectal lesion resection. R0 resection rates and adverse events were comparable across techniques, which is reassuring and supports the value of both approaches in modern ESD practice. The most notable signal was procedural efficiency: UW-ESD was the only strategy associated with significantly faster dissection compared with T-ESD and conventional ESD.
We believe this adds an important piece to the current literature. In a field where technical success is often measured not only by curative resection but also by procedural flow and feasibility, speed matters—particularly for wider adoption outside expert Eastern centers. At the same time, our study also reinforces that there is probably no single “winning” strategy for every lesion. The future may lie in a more tailored approach, selecting or combining techniques according to lesion characteristics, fibrosis, location, and scope stability. Head-to-head randomized trials, especially in Western settings, are now needed to validate these findings and better define how these techniques should be integrated into routine practice.
More broadly, this study reflects an ongoing shift in endoscopy: the goal is no longer simply to perform ESD, but to perform it in a smarter, more adaptable, and more efficient way. That is where meaningful innovation is happening.
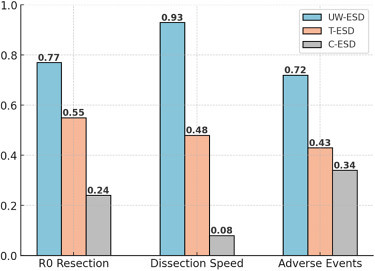
SUCRA score ranking. R0 resection: UW-ESD ranked highest (SUCRA: 0.77) compared with T-ESD (SUCRA: 0.55) and C-ESD (SUCRA: 0.24), dissection speed: UW-ESD ranked highest (SUCRA: 0.93) compared with T-ESD (SUCRA: 0.48) and C-ESD (SUCRA: 0.08), safety: UW-ESD ranked highest (SUCRA: 0.72) compared with T-ESD (SUCRA: 0.43) and C-ESD (SUCRA: 0.34). C-ESD, Conventional endoscopic submucosal dissection; SUCRA, surface under the cumulative ranking curve; T-ESD, traction-assisted ESD; UW-ESD, underwater ESD.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
