
Post written by Sneh Sonaiya, MD, from the Department of Internal Medicine, University of Nevada Las Vegas, Las Vegas, Nevada, and Babu P. Mohan, MD, from the University of Central Florida School of Medicine and Orlando Gastroenterology PA, Orlando, Florida, USA.

Although prophylactic clipping is commonly used after EMR of large colon polyps to reduce delayed postpolypectomy bleeding, its cost-effectiveness has not been well established. Our study evaluated whether prophylactic clipping after EMR of large nonpedunculated colon polyps (≥20 mm) is cost-effective compared with no clipping.
Data from randomized controlled trials on the effectiveness of prophylactic clipping in preventing delayed postpolypectomy bleeding have been mixed. Use of endoscopic clips adds significant expense, especially in standalone surgery centers. We felt it was important to clarify when prophylactic clipping provides true economic value in clinical practice, especially as endoscopy continues to shift toward more cost-conscious, value-based care. Our goal was to identify the clinical scenarios where clipping is cost-saving or cost-effective and to define practical thresholds for clip cost and use.
Our study adds an economic perspective to a clinical question that endoscopists face daily: when does prophylactic clipping after EMR actually provide value? Using pooled randomized trial data, we show that universal clipping is not cost-effective, but selective clipping in high-risk settings clearly is.
Prophylactic clipping was cost-saving for large (≥20 mm) proximal lesions, cost-effective for very large polyps (≥40 mm) regardless of location, and cost-saving in patients on antithrombotic therapy when clip use is limited (≤2 clips). We also identified practical thresholds showing that clipping remains economically favorable when per-clip costs are ≤$217 or when ≤4 clips are used in proximal lesions.
Overall, these findings support a targeted, risk-stratified approach to prophylactic clipping—based on lesion size, location, clip use, and antithrombotic medication use—rather than routine clipping for all EMR cases. Our findings emphasize the need for reducing clip costs and developing reimbursement pathways to support the broader adoption of hemostatic clips in clinical practice, particularly for high-risk scenarios when clipping has demonstrated economic and clinical benefits. Future studies should focus on refining patient-level bleeding risk prediction, incorporating real-world practice patterns, and evaluating strategies to reduce clip costs and optimize use to further improve both clinical outcomes and economic value in EMR.
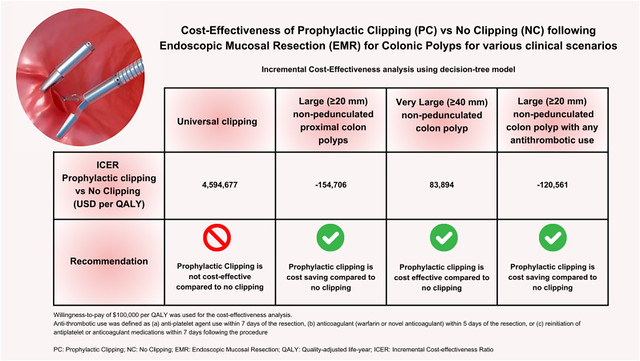
Schematic diagram of cost-effectiveness results for prophylactic clipping versus no clipping after EMR across various clinical scenarios.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
