
Post written by Ernesto Robalino Gonzaga, MD, from Gastroenterology and Hepatology, AdventHealth Medical Group, and Dennis Yang, MD, from the Center for Interventional Endoscopy, AdventHealth, Orlando, Florida, USA.

Our study evaluated the clinical outcomes of endoscopic submucosal dissection (ESD) for residual neoplasia after incomplete endoscopic resection of large nonpedunculated colorectal polyps. Specifically, we compared outcomes of ESD performed as salvage therapy after prior failed endoscopic resection with outcomes with treatment-naïve lesions using a large multicenter propensity score–matched cohort. The primary aim was to assess technical success, safety, and recurrence rates to better define the role of ESD in managing these challenging colorectal lesions.
Incomplete resection of large colorectal lesions is a common clinical problem, and many patients referred for advanced endoscopic therapy in Western practice have undergone prior manipulation, including attempted resection, biopsy, or tattooing. These interventions often result in submucosal fibrosis, which increases procedural complexity and may affect outcomes. However, data from Western centers on the safety and effectiveness of ESD as a salvage strategy in this setting remain limited.

We felt this study was important to address a critical gap in evidence and help guide clinical decision-making. Understanding whether ESD remains safe and effective after failed resection can support organ-preserving treatment strategies, reduce unnecessary surgical referrals, and inform guideline-based management of residual colorectal neoplasia.
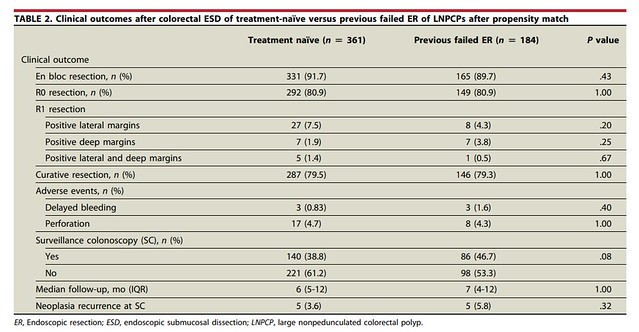
In this large multicenter propensity score–matched study, we found that ESD performed after a failed endoscopic resection achieved comparable en bloc and R0 resection rates, adverse event rates, and recurrence outcomes when compared with ESD for treatment-naïve lesions. Despite concerns that prior manipulation and fibrosis may compromise outcomes, salvage ESD remained technically feasible and clinically effective when performed at expert centers.
These findings provide important real-world evidence supporting the role of ESD as a viable organ-preserving treatment option for residual colorectal neoplasia. Our results reinforce current guideline recommendations that include ESD among potential management strategies for these difficult lesions and help clarify its role in Western practice.
Future studies should focus on prospective comparisons between ESD and alternative salvage techniques, better characterization of fibrosis severity, optimization of patient selection, and long-term surveillance outcomes. In addition, strategies to minimize unnecessary lesion manipulation before referral may further improve outcomes.
Our study highlights the importance of multidisciplinary collaboration and referral to experienced centers for complex colorectal lesions. As adoption of advanced endoscopic resection continues to expand in Western practice, defining appropriate indications and optimizing outcomes for challenging lesions will remain essential to improving patient care and reducing the need for surgical intervention.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
