
Post written by Yassmin Hegazy, MD, from the Department of Medicine and the Department of Internal Medicine, University of Alabama Birmingham Hospital, Birmingham, Alabama, USA.

Our case is about a 73-year-old man with a history of GERD and diabetes mellitus who presented with a 1-week history of hematochezia with associated nausea, vomiting, diarrhea, and epigastric pain.
His CT imaging showed a pulmonary mass and a duodenocolonic fistula in the second part of the duodenum. Upper GI endoscopy displayed a 10-mm fistula in the first and second portions of the duodenum with opening into the right side of the colon and an infiltrative mass past the duodenal bulb with biopsy positive for invasive adenocarcinoma.
Considering a palliative approach, we placed a Niti-S (Taewoong Medical, Los Angeles, CA) bare-type covered metal luminal esophageal stent under fluoroscopic guidance that was anchored proximally by the endoscopic placement of 2 interrupted sutures to prevent distal migration.
The patient was seen 3 weeks postprocedure with improvement in symptoms, and imaging revealed a second primary lung malignancy.
This video highlights a palliative and endoscopic approach to stenting a duodenocolonic fistula in a patient with metastatic disease. Malignant duodenocolonic fistulas can cause rapid nutritional deficiencies and severe symptoms, including diarrhea and abdominal pain. An endoscopic approach by placing a covered duodenal stent with stent fixation would allow for a less-invasive alternative to surgery while providing symptom relief, especially in a palliative situation.
Our study demonstrates a palliative approach to treating patients with significant disease burden from malignant duodenocolonic fistulas. Although alternative endoscopic approaches, such as through-the-scope or over-the-scope clips, can be used for enteral fistula closure, they have a higher likelihood of dislodging given their smaller size relative to the fistula.
In addition, primary endoscopic suturing of the defect can have a higher probability of the sutures to fail and dehisce given the friability associated with the tumor, and it can ultimately provide minimal relief.
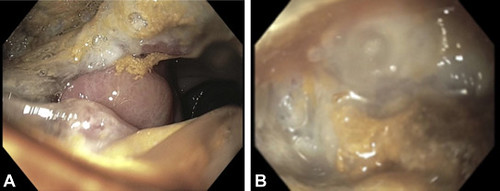 A, A medium fistula found in the first portion of the duodenum and in the second portion of the duodenum, opening into the right side of the colon, at the region of hepatic flexure. B, Medium-sized fungating mass in the first and second portion of the duodenum.
A, A medium fistula found in the first portion of the duodenum and in the second portion of the duodenum, opening into the right side of the colon, at the region of hepatic flexure. B, Medium-sized fungating mass in the first and second portion of the duodenum.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
