
Post written by Yervant Ichkhanian, MD, from the Department of Medicine, Henry Ford Hospital, Detroit, Michigan, USA.

A 67-year-old man with a history of total gastrectomy before Roux-en-Y esophagojejunostomy reconstruction in the setting of gastric adenocarcinoma presented with extensive choledocholithiasis with a benign terminal bile duct stricture.
In our case, the patient underwent jejuno-enterostomy using a lumen-apposing metal stent (LAMS) to facilitate cholangioscopy and lithotripsy.
In patients with surgically altered upper GI anatomy and complex pancreaticobiliary pathologies that might require multiple interventions, enteroscopy-assisted ERCP becomes technically challenging, and the length of the devices often limit therapeutic interventions. Patients are often offered invasive endoscopic, percutaneous, or even surgical management approaches.
The patient preferred the invasive and technically challenging endoscopic approach, which was the creation of an enteroenterostomy using a LAMS to access the pancreaticobiliary anastomosis site, given that it allowed advanced interventions (such as cholangioscopy with electrohydraulic lithotripsy) without the need for external drainage or surgery and with acceptable technical and clinical outcomes.
In patients with surgically altered anatomy who present for choledocholithiasis with extensive stone burden, it is reasonable to proceed with the creation of EUS-guided de novo enteroenterostomy using LAMSs, as it will allow a wider range of management tools.
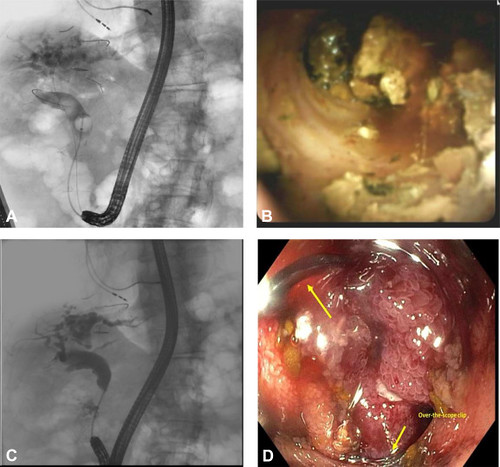 ERCP with cholangioscopy and electrohydraulic lithotripsy through the EUS-guided jejuno-jejunostomy. A, Fluoroscopic view of a diagnostic cholangiogram indicating the multiple large stones. B, Endoscopic image during cholangioscopy. C, Cholangiogram post–electrohydraulic lithotripsy indicating the absence of stones. D, Endoscopic closure of the jejuno-jejunostomy with argon plasma coagulation and an over-the-scope clip.
ERCP with cholangioscopy and electrohydraulic lithotripsy through the EUS-guided jejuno-jejunostomy. A, Fluoroscopic view of a diagnostic cholangiogram indicating the multiple large stones. B, Endoscopic image during cholangioscopy. C, Cholangiogram post–electrohydraulic lithotripsy indicating the absence of stones. D, Endoscopic closure of the jejuno-jejunostomy with argon plasma coagulation and an over-the-scope clip.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
