
Post written by Emily R. Jonica, MD, from the Division of Gastroenterology and Hepatology, University of Colorado Anschutz Medical Campus, Aurora, Colorado, USA.

In our video, we showcase the use of per-oral pancreatoscopy (POP) with holmium laser therapy during ERCP to address a nontraversable severe stricture and upstream large main pancreatic duct (MPD) stone in the body of the pancreas causing pain and recurrent bouts of pancreatitis.
Laser stricturoplasty was the focus of the initial POP session, permitting deep guidewire access across the stone and successful bridging with a stent to the tail. Follow-up POP with holmium laser using stone fragmentation settings was then successful in achieving ductal clearance.
Our case highlights a dilemma of complex MPD stone management in this difficult patient population. Coexisting long or severe strictures just downstream from the impacted stone with inability to traverse the stone with either contrast or a wire may lead to technical failure. For example, plastic or metal passage dilators are useful only if a guidewire can cross the obstruction. Endoscopists may encounter this scenario and feel that only a surgical option, which usually entails gland resection, is required.
Although extracorporeal shock wave lithotripsy is an effective method for breaking stones, our opinion is that ERCP should be pursued to clear the duct of stones and treat underlying strictures to reduce the risk of stone recurrence.
Finally, our video displays the radiographic, fluoroscopic, pancreatoscope images and technique of POP with laser therapy in overcoming the mentioned barriers to promote successful endotherapy for difficult stone cases, preserving an obstructed pancreatic gland and avoiding the need for surgery.
In MPD stone disease, POP with laser therapy can treat obstructing strictures to improve access to symptomatic stones in the same session. The location of obstruction is a determining factor in patient selection for pursuing laser therapy because if there is significant upstream parenchymal atrophy, the advantages of salvaging the gland may be limited.
Although location of the MPD obstruction in the head may cause difficulty with positioning the pancreatoscope, we find that obtaining even superficial access into the pancreatic duct orifice with the tip of the scope is often sufficient for experienced endoscopists to perform lithotripsy. This scenario can require freehand cannulation of the pancreatoscope with the laser (or EHL) fiber minimally protruding from the working channel, given the acute angulation.
In addition, passage of the pancreatoscope also is often facilitated by balloon dilation of downstream strictures. If soft-tissue dissection is planned and known prior to the procedure, our preference is to use the continuous wave thulium laser, but in the case of stone therapy, adjusting settings (as in our case) permits both soft-tissue dissection/ablation and stone lithotripsy.
This is a complex patient population, and the ability to expand the use of laser to include soft-tissue dissection can help treat strictures and improve pancreatoscope positioning to target upstream obstructing stones. This often requires multiple sessions. Therefore, pre-procedure patient counselling is necessary prior to commencing therapy.
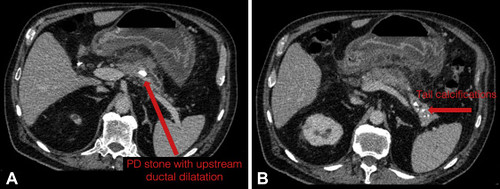 Index CT scan from referring hospital, demonstrating 15-mm intraductal stone in the body of the main pancreatic duct and upstream ductal dilatation (A). Parenchymal tail calcifications are also noted (B).
Index CT scan from referring hospital, demonstrating 15-mm intraductal stone in the body of the main pancreatic duct and upstream ductal dilatation (A). Parenchymal tail calcifications are also noted (B).
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
