
 Post written by Yunlu Feng, MD, and Aiming Yang, MD, from the Department of Gastroenterology, Peking Union Medical College Hospital, in Beijing, China
Post written by Yunlu Feng, MD, and Aiming Yang, MD, from the Department of Gastroenterology, Peking Union Medical College Hospital, in Beijing, China
Our article reported a 34-year-old male Chinese patient who presented with feeling of incomplete defecation and abdominal pain for more than 10 years. Colonoscopy showed a single rectal ulcer. Magnetic resonance imagine showed localized rectal wall thickening. We performed probe-based confocal laser endomicroscopy (pCLE) of the lesion. The images showed dark thickened epithelium and decreased goblet cells, villous architecture, branch-like crypts, while dilated vessels and decreased crypt/stroma ratio with reticular gray pattern in stroma. Endoscopic biopsies of the lesion showed fibromuscular obliteration of the lamina propria, glandular crypt abnormalities such as hyperplasia, and dilation of small vessels. SRUS was diagnosed with combination of symptoms, colonoscopic findings and histopathological abnormalities. 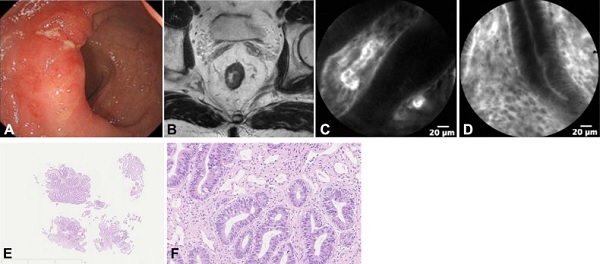
Figure 1. A, Colonoscopic image showing an irregular ulcer with surrounding edema and erosion in the rectum under white light. B,Magnetic resonance image showing localized wall thickening in the middle part of the rectum. C, D, Probe-based confocal laser endomicroscopic image showing (C) dark thickened epithelium and dilatated vessels and (D) villous architecture and decreased crypt/stroma ratio with reticular gray pattern in stroma. E, F, Histologic views of the biopsy specimen showing fibromuscular obliteration of the lamina propria, hyperplasia of epithelium, and dilatation of small vessels at (E) low power (H&E, orig. mag. ×1.78) and (F) high power (H&E, orig. mag. ×20).
Although many benign or malignant colorectal diseases such as adenoma, hyperplastic polyp, colitis, and cancer have well-described characteristics under pCLE, little is known about the mucosal changes of SRUS. Our pCLE images showed an agreement with the histological result, and had unique characteristics different from other diseases.
From our experience, the typical findings of SRUS under pCLE are goblet cell depletion, branch-like crypts, microvascular alterations without fluorescein leakage and the most important one, decreased crypt/stroma ratio. pCLE can be an effective diagnostic modality of SRUS and other colorectal diseases by real-time histology and guiding more precise biopsy.
