
 Herbert C. Wolfsen, MD, from the Division of Gastroenterology and Hepatology, Mayo Clinic, Jacksonville, Florida, USA describes this video case “Incarcerated, retroflexed endoscope associated with a paraesophageal hernia.”
Herbert C. Wolfsen, MD, from the Division of Gastroenterology and Hepatology, Mayo Clinic, Jacksonville, Florida, USA describes this video case “Incarcerated, retroflexed endoscope associated with a paraesophageal hernia.”
An elderly woman underwent upper endoscopy in our ASC to evaluate GERD symptoms and dysphagia in setting of PEH. Unfortunately, the endoscope could not be easily passed through the PEH into the distal stomach. Instead, the endoscope re-intubated the esophagus in retrograde fashion becoming entrapped. The endoscope could not be successfully advanced or withdrawn.
I made sure the patient was well sedated and asked for help from 2 other endoscopists. We then disconnected the entrapped endoscope from the video processor and passed a second endoscope along the entrapped scope, as I had been taught by Richard Kozarek during my time with him as an internal medicine resident in Seattle some thirty years ago.
We then attempted to use the 2nd scope to abut the trapped scope to advance them. This was not successful however. So, we used the most readily available device, a biopsy forcep, to “bridge” the 2 scopes. The forceps were passed only a few centimeters into the device channel of the trapped scope, to ensure there was no damage to the equipment. With these scopes bridged together, they would now move along the same vector to permit us to advance them distally into the stomach. At that point, the first scope unfurled and could be withdrawn. We uneventfully completed the diagnostic exam with the second endoscope. The patient was then transferred to the ASC recovery area in good condition with no subsequent procedure-associated problems. 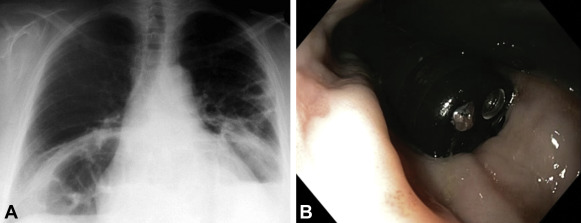
Figure 1. A, Chest radiograph demonstrating retrocardiac mass consistent with a paraesophageal hernia. B, Endoscopic view confirming that the trapped endoscope was retroflexed in the tubular esophagus.
This is probably a very uncommon problem, as it has never happened to me before in my 20+ year career. As soon as I recognized the situation, I started the video capture. Even though I was not entirely sure how the case would turn out, I expected the video footage to be educational for all GI physicians.
What can other endoscopists learn from my experience? Remain calm. Keep the patient well sedated. Ask for help from your colleagues. And remember what you mentors taught you!
Find more VideoGIE cases online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.

Dear Dr Wolsen, Thanks for the case. I encountered a similar case some 17 years ago when a colleague managed to impact the gastroscope in the oesophagus in the J position. Our patient did not have a paraoesophageal hernia. I was called to assist and we did exactly what you did, using a biopsy forceps to bridge the two ‘scopes and then pushing down to dis-impact the first scope.