
 James H. Tabibian, MD, PhD, from the Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota, USA shares this VideoGIE case “Endoluminal stenting via the suture-assisted flange engagement technique.”
James H. Tabibian, MD, PhD, from the Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota, USA shares this VideoGIE case “Endoluminal stenting via the suture-assisted flange engagement technique.”
Gastrointestinal endoscopists are now more than ever encountering clinical scenarios where they are asked to provide endoscopic diversion or bridging of a leak site with fully-covered self-expanding metallic stents (cSEMSs). In some cases, the length of the conduit needed may exceed that of commercially available cSEMSs, which currently have a maximum unconstrained length of 15 cm. Additional issues which may exist when needing to bridge such long distances include unfavorable buckling forces (precluding successful overlapping of the cSEMS) and insufficient wall:stent apposition and resulting in stent migration. To overcome these issues, we developed a technique for extended alimentary tract bridging with tandem cSEMS via the suture-assisted flange engagement (SAFE) technique which we have used in a variety of circumstances (eg, Ivor-Lewis anastomotic disruption, duodenal leak in the setting of necrotizing pancreatitis).
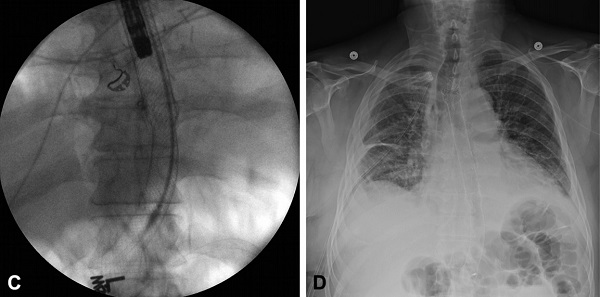
Figure 1. C, Fluoroscopic view of 2 contiguous cSEMSs via the suture-assisted flange engagement (SAFE) technique. D, Radiographic image of the 28-cm esophagoduodenal cSEMS conduit.
In brief, the sheath of a cSEMS (eg, a 15 cm WallFlex [Boston Scientific, Marlborough, MA]) is slightly retracted ex vivo to expose its distal flange loops, through which a continuous purse-string suture is fashioned to constrain the flange diameter. This is reinforced with interrupted sutures, and the flange is re-sheathed. The modified cSEMS is then deployed with its proximal (ie, unsutured) flange above the anastomosis and, if possible, EndoCinch-sutured (Bard, Billerica, MA) in place. Next, a second cSEMS is deployed through the first cSEMS with its proximal flange carefully positioned within the constrained distal flange of the first stent (Figure 1C). This ~28 cm stent conduit (Fig. 1D) can then be atraumatically removed after the desired duration of endoscopic stenting.
To summarize, the SAFE technique provides endoscopists a means to safely and effectively provide extended-range endoscopic stent conduits beyond the capabilities of currently availabe cSEMSs and thereby facilitate underlying tissue healing.
This VideoGIE shares with GI endoscopists a practical, safe, and effective technique to treat alimentary tract disruptions, leaks, and fistulae which otherwise cannot be adequately managed with currently available metallic (or other) stents.
Find more VideoGIE cases online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.

Ever since the inception of metallic stenting in the GI tract, I’ve always wondered why as GI Endoscopists we couldn’t have longer stenting capabilities. This neat and practical report addresses that very issue and permits nearly a 1-foot long covered conduit. Nice work– our surgeons may come knocking on my door for this…!
Thank you for the thoughtful comment, MW.
This technique is tremendously helpful and may supplant the need for more invasive treatments (e.g. surgery) in carefully selected patients. The importance of careful planning, including a multidisciplinary approach, discussion with the patient, and technical preparedness, should be emphasized.
If your colleagues are requesting the SAFE technique, it’s likely they are hesitant to (re-)operate, and thus having the capability to implement it can prove to be quite useful, as it has at our institution.
Neat article and technique. I was wondering, including yourself, how many endoscopists at Mayo Clinic in Rochester know how to use/perform the SAFE technique?
Raj, thank you for your post.
I’m actually no longer at Mayo (currently at Penn, but moving to UC Davis in June); however, one of my mentors, Dr. Nav Buttar, is still there and was the one who developed the technique. Although he’s the only endoscopist at Mayo who performs SAFE stenting, I’m sure others in the advanced group could pick up the technique as needed.
Cheers