
Post written by Shigenori Masaki, MD, from the Department of Surgery and Gastroenterology, Miyanomori Memorial Hospital, Sapporo, Japan.

What if endoscopists could examine their own gastrointestinal tract?
We investigated the optimal method for gastrointestinal endoscopists to perform esophagogastroduodenoscopy (EGD) on themselves, evaluating the insertion route (transnasal vs transoral), body position, endoscope maneuverability, and monitor visibility.
Gastrointestinal endoscopists routinely perform EGD on patients; however, when they experience gastrointestinal symptoms themselves, they also may require EGD. Because of their busy clinical schedules, endoscopists may neglect their own symptoms and delay evaluation. Some may feel reluctant to ask colleagues to perform the procedure on them.
In addition, those working in rural or underserved areas may not have access to another physician capable of performing EGD. Traveling to a distant hospital for the procedure can be burdensome, possibly resulting in them not undergoing EGD at all.
Such situations are a reality in Hokkaido, Japan, where I practice. Because of the large distances between cities, individuals may need to travel tens to hundreds of kilometers to undergo EGD.
Therefore, I believe that, depending on individual circumstances, it may be necessary for endoscopists to perform EGD on themselves to monitor their own gastrointestinal health. To provide optimal care for patients, endoscopists themselves also must maintain good health.
Over the past 20 years, I have repeatedly performed EGD on myself using transnasal or transoral endoscopy in various positions, including the left lateral, supine, sitting, and standing positions, to determine the optimal approach.
To our knowledge, transnasal endoscopy in the standing position represents the most suitable method. Transnasal endoscopy is associated with a reduced gag reflex, and the standing position offers advantages in terms of maneuverability and monitor visibility. In my experience, the sitting position was associated with a sense of gastric compression and reduced ease of scope manipulation, whereas the standing position was more comfortable and practical.
However, some individuals may find the sitting position more suitable. Therefore, it is important for each endoscopist to identify the method that works best for them.
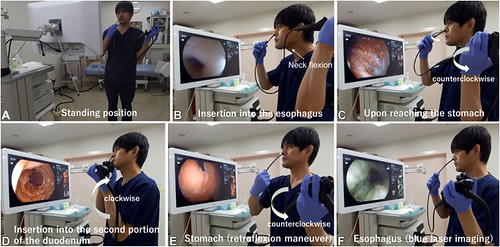
A, Procedure for self-performed transnasal esophagogastroduodenoscopy in the standing position (demonstrated by S. Masaki). B, Dotted arrow indicates the direction of neck flexion to facilitate passage of gastroscope into esophagus seen on the monitor. C-E, Thick rotational arrow indicates the direction of endoscope rotation. C, Upon reaching the stomach, counterclockwise torque with the left arm was needed to reach duodenum. D, To enter the second portion of the duodenum from the bulb, clockwise torque with the left arm was needed. E, Retroflexion in the stomach was possible with counterclockwise torque. F, Blue-laser imaging used to assess esophagus.
Visit iGIE’s Facebook, X/Twitter, LinkedIn, Instagram, and YouTube accounts for more content from the ASGE peer-reviewed journal that launched in December 2022 and has been PubMed indexed.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
