
Post written by Amol Bapaye, MD (MS), FASGE, MSGEI, FISG, FJGES, and Sanjana Bhagwat, MD, DNB, from Deenanath Mangeshkar Hospital and Research Center, Pune, India.

We highlight a case of a 74-year-old woman presenting with a 3.8- x 3.3-cm exophytic gastrointestinal stromal tumor on the lesser curvature that was treated using a unique strategy and technique.
The strategy: After histological confirmation, the tumor was first downsized using cytoreductive chemotherapy (imatinib 400 mg over 3 months), followed by endoscopic resection.
The technique: After submucosal elevation, a horizontal incision was taken proximal to the tumor to create a submucosal tunnel. Full-thickness myotomy was performed proximal to the tumor, and the peritoneum was entered to approach the lesion from the serosal aspect. We achieved prophylactic coagulation and division of the serosal vessels along with adhesiolysis before commencing dissection. Using clip-and-line traction, we carefully dissected the tumor from the muscle layer while avoiding breach of the capsule.
While applying continuous traction on the clip and line, we performed the final resection of the remnant muscle attachment using a snare, and the tumor was delivered through the tunnel after extending the myotomy. Mucosal incision was closed by endoscopic suturing. The specimen was retrieved using a double-channel scope with grasping forceps and snare.
The patient was hospitalized for 72 hours. Follow-up at 1 month confirmed complete healing, with CT scan at 6 months showing no residual or recurrent lesion.
Endoscopic resection of exophytic gastrointestinal stromal tumors remains an infrequent choice in clinical practice. This is largely because of 2 significant technical challenges: (1) bleeding from the serosal surface that can be difficult to control from the intraluminal aspect and (2) risk of losing the tumor into the peritoneal cavity. In our featured video, we demonstrate a novel technique–endoscopic tunneling and subserosal dissection, designed to mitigate these risks through a natural orifice transluminal endoscopic surgery approach.
Other endoscopists can learn from this experience:
- Use of neoadjuvant imatinib–Effective reduction in size of the tumor from 3.8 x 3.3 cm to 2.8 x 2.6 mm in 3 months improves ease and success of endoscopic resection.
- Prophylactic hemostasis–Approaching the tumor via the natural orifice transluminal endoscopic surgery window allows for prophylactic management of serosal vessels before they become a bleeding risk during dissection.
- Controlled retrieval—The use of traction during final resection prevented loss of the tumor into the cavity. Specimen retrieval using rat tooth and snare avoided breach of the capsule during retrieval.
- Tunneling safety—The submucosal tunnel provides a good entry point and adequate closure of the defect and acts as a seal, giving additional protection against postprocedural leaks.
To our knowledge, the endoscopic tunneling and subserosal dissection approach offers a robust alternative for managing exophytic lesions previously relegated to laparoscopic or open surgery. Watch the full step-by-step approach and dissection.
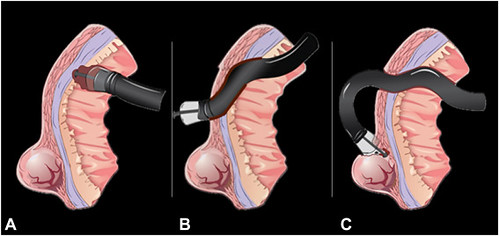
Cartoon drawing showing a submucosal tunnel proximal to the tumor and proximal full-thickness myotomy (A), transtunnel peritoneoscopy and subserosal dissection (B), and a tumor delivered through the tunnel into the stomach (C).
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
