
Post written by Varun Jain, MD, MBA, and Sultan Mahmood, MD, FASGE, from the Division of Gastroenterology, Hepatology, and Nutrition, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA.

We present a case of endoscopic mesorectal dissection (EMD) performed for staging and potential treatment of a residual rectal adenocarcinoma following incomplete hot snare polypectomy. A 67-year-old man underwent colonoscopy after a positive multitarget stool DNA test result, which revealed a 2-cm sessile polyp 12 cm from the anal verge. Pathology demonstrated invasive adenocarcinoma with positive vertical margins. Cross-sectional imaging showed no lymphadenopathy but could not determine depth of invasion.
Given the lesion’s proximal location and technical challenges encountered during attempted local excision, EMD was selected. After marking the lesion, submucosal injection with methylene blue was performed followed by circumferential incision. A full-thickness myotomy was completed to expose the perirectal fat, allowing en bloc resection of a 35-mm specimen. The defect was closed with running sutures using the OverStitch device (Boston Scientific Corporation, Marlborough, Mass, USA). Final pathology revealed moderately differentiated pT2 adenocarcinoma with R0 margins.

We felt this case highlights the expanding role of advanced endoscopic techniques in rectal cancer management. EMD allows precise full-thickness resection and accurate pathological staging while preserving organ integrity. In challenging anatomic locations, such as proximal rectal lesions behind folds or along the anterior wall, traditional surgical approaches or transanal techniques may be limited. This video displays how EMD can safely achieve en bloc R0 resection in such cases and serve as both a diagnostic and potentially therapeutic modality.
This case illustrates that EMD can be a technically feasible and safe alternative to local surgical excision in select patients. Key learning points include:
- Careful lesion marking and submucosal injection for orientation.
- Controlled full-thickness dissection into the mesorectum.
- Recognition of perirectal fat planes to maintain safe margins.
- Reliable defect closure using endoscopic suturing.
EMD provides wide-field exposure, enabling precise differentiation between tumor and fibrosis, and can facilitate accurate staging with en bloc R0 resection.
EMD represents a minimally invasive, organ-preserving strategy that may complement multidisciplinary rectal cancer management. As data evolve regarding surveillance strategies and systemic therapies, EMD may increasingly serve as an important tool for staging and treatment in carefully selected patients.
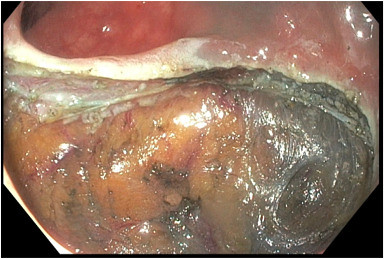
Full-thickness defect following endoscopic mesorectal dissection of the rectal cancer lesion, demonstrating complete excision of the lesion with exposure of the perirectal fat.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
