
Post written by Fatih Aslan, MD, from Gastroenterology and Advanced Endoscopy, Koc University Hospital, Istanbul, Turkey.

This video presents a case of multitunnel endoscopic submucosal dissection (ESD) followed by endoscopic suturing in a patient with an approximately >30-cm-long circumferential laterally spreading tumor located in the rectum.
A 51-year-old woman presenting with diarrhea underwent colonoscopic evaluation, which revealed a large circumferential laterally spreading tumor extending proximally from approximately 4 cm above the anal verge. The procedure was performed with the patient under general anesthesia, and en bloc resection was achieved using the multitunnel technique. The resected specimen measured 324 × 214 mm.
Following ESD, the extensive mucosal defect was closed using the OverStitch endoscopic suturing system (Boston Scientific, Marlborough, Mass, USA). Histopathological examination demonstrated a tubulovillous adenoma with high-grade dysplasia, with negative resection margins. No early postprocedural adverse events were observed, and long-term follow-up showed no evidence of recurrence or stricture formation.
This video was driven by fundamental questions: can a 33-cm circumferential resection truly challenge the functional limits of ESD, and where should we draw the line between technical feasibility and luminal preservation? These considerations formed the starting point for sharing this case.
It represents not only a technically demanding procedure but also a shift in how we approach ultra-large circumferential resections. With large lesions—particularly those exceeding 10 cm with near-circumferential or fully circumferential involvement—ESD presents unique challenges, including limited luminal space, restricted visualization, and constant risk of losing orientation.
To overcome these difficulties, we had the opportunity to once again demonstrate the value of the multitunnel technique, which we first presented at the 2016 American Society for Gastrointestinal Endoscopy World Cup at Digestive Disease Week and later published about. Despite numerous innovations and new approaches in saline- and traction-based ESD techniques over the past decade, we believe that tunnel-based strategies continue to play a critical role, especially with large circumferential lesions. This approach helps maintain orientation, improves procedural control, and may positively influence overall efficiency.
Another important aspect arises when the resection length reaches extreme dimensions: the discussion extends beyond dissection itself and shifts toward functional outcomes—particularly stricture prevention. Presenting this experience at the 2025 World Cup and sharing it as a publication was important to us because it shows how advanced endoscopic suturing strategies can be integrated into complex ESD workflows to help preserve luminal function.
In regard to what other endoscopists can learn from our experience, first, with large lesions, accurate staging followed by a carefully planned resection strategy tailored to the anatomical location is a key determinant of procedural success.
Second, the limits of ESD are rarely defined by resection size alone; they are shaped by planning, defect management, and postprocedural strategy. Large circumferential dissections require a different mindset, anticipating fibrosis, tissue tension, and healing dynamics from the very beginning of the procedure.
Finally, suturing should not be viewed solely as a method to prevent short-term adverse events but rather as a component of functional reconstruction. Even with very long resections, a well-planned suturing strategy may contribute to more favorable tissue remodeling and potentially reduce stricture formation.
The primary focus of this work is to explore the evolving role of endoscopic suturing after extensive resections and its potential long-term benefits. Our aim is not to define absolute limits but rather to question where those limits may lie and how procedural strategy can influence outcomes.
Ongoing case-controlled studies with long-term follow-up are underway, and we hope these data will provide a clearer framework for understanding when and how suturing may be most beneficial in large circumferential ESD defects.
Ultimately, the goal of innovation is not only to solve exceptional cases but also to improve everyday clinical practice. Techniques should not remain limited to extreme scenarios; they must be adaptable to real-world settings.
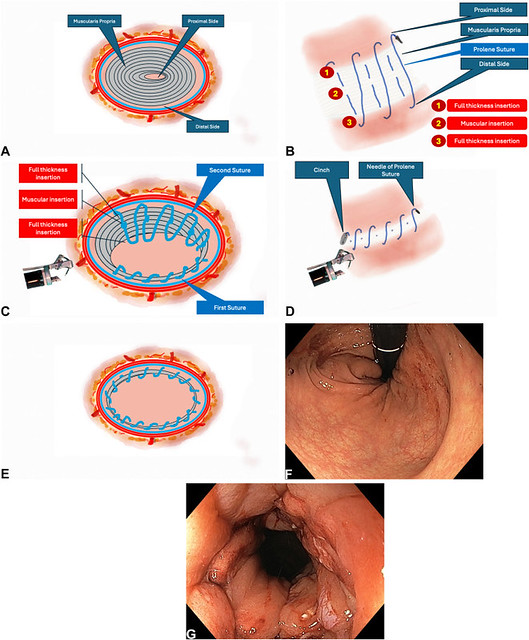
A, Schematic view of the resection area. B, Schematic view of the suturing strategy. C, Schematic view of the suturing strategy. D, Schematic view of the postprocedural suturing strategy. E, Schematic view of the postprocedural suturing strategy. F, Endoscopic view of the resection area in retroflexed position after suturing. G, Endoscopic view of the resection area in straight position after suturing.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
