
Post written by Taranika Sarkar Das, MD, from The Brooklyn Hospital, Brooklyn, New York, and Matheus Franco, MD, PhD, from the Division of Gastroenterology and Human Nutrition at the University of Texas Health San Antonio and UT Health San Antonio’s Multispecialty and Research Hospital, San Antonio, Texas, USA.

We present a case of a 67-year-old man with prior T3N1M0 rectal adenocarcinoma treated with neoadjuvant chemoradiotherapy followed by proctosigmoidectomy. Surveillance later revealed a 3.5-cm granular, mixed-nodular laterally spreading tumor located directly over the rectal anastomotic staple line. Advanced imaging with narrow-band imaging and chromoendoscopy demonstrated features consistent with advanced neoplasia, without clear deep submucosal invasion.
Given the dense postsurgical fibrosis and presence of retained staples, we performed a novel “saline-tunneling” endoscopic submucosal dissection (ESD). This technique combines continuous saline immersion with submucosal tunneling, allowing stable visualization, improved optical magnification, reduced electrosurgical smoke, and buoyancy-assisted dissection. A controlled tunnel was created under sustained immersion, enabling safe exposure and removal of obstructing staples while maintaining precise plane control.
En bloc resection was achieved in 118 minutes without adverse events. Histopathology confirmed tubulovillous adenoma with high-grade dysplasia and negative margins. At 1-year follow-up, there was no recurrence.
Anastomotic lesions are among the most technically challenging scenarios in colorectal ESD because of fibrosis, altered anatomy, and metallic staples. These cases are often referred for repeat surgery. We felt it was important to show that a carefully executed saline-tunneling strategy can provide a safe and effective minimally invasive alternative in highly select patients.
To our knowledge, this is the first case report combining continuous saline immersion with tunneling ESD in a postsurgical colorectal setting. This case highlights several key lessons:
- Continuous saline immersion improves visualization, plume washout, and electrosurgical predictability—especially near metallic staples.
- A true submucosal tunnel provides stability and bidirectional access across fibrotic anastomotic tissue.
- Controlled staple exposure and removal can be performed safely within a stable immersed field.
- Complex anastomotic lesions may be amenable to advanced endoscopic therapy when performed by experienced operators.
Although this is a single case, it suggests that saline-tunneling ESD may broaden therapeutic options for challenging colorectal lesions in surgically altered anatomy.
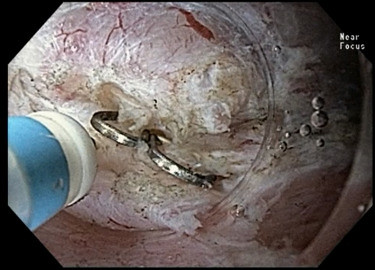
Deep submucosal dissection at the anastomotic line exposed several surgical staples, which were subsequently removed to complete the resection.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
