
Post written by Partha Pal, MD, DNB, MRCP (UK), FASGE, from the Department of Medical Gastroenterology, Asian Institute of Gastroenterology, Hyderabad, India.
This video demonstrates a staged endoscopic stricturotomy using the segmental layered incision and circumferential endoscopic dissection (SLICE) technique in a patient with a long, tight fibrotic colonic stricture at the splenic flexure. The stricture was associated with distorted anatomy and significant luminal narrowing, making conventional radial incision and cutting potentially unsafe.
Drawing principles from endoscopic submucosal dissection, the SLICE technique involves shallow, controlled circumferential dissection of fibrotic tissue in sequential layers, performed over multiple sessions. This video highlights stepwise exposure of the fibrotic ring, use of focal mucosectomy to define planes, visual and tactile safety cues, and progressive lumen remodeling without deep mural injury. The stricture was successfully traversed after staged dissection with no bleeding or perforation, and durable luminal patency was confirmed on follow-up.
Complex fibrotic strictures remain one of the most challenging scenarios in therapeutic endoscopy, particularly when they are long, angulated, or located in high-risk colonic segments. Although endoscopic balloon dilation and conventional stricturotomy are effective in select cases, their durability and safety can be limited in the setting of advanced fibrosis.
We felt it was important to showcase an approach that moves beyond simple lumen expansion toward endoscopic reconstructive surgery, where the goal is controlled, stepwise remodeling of the stricture architecture. The SLICE technique demonstrates how principles adapted from endoscopic submucosal dissection can be applied to reconstruct complex luminal strictures in a precise, anatomy-respecting, and staged manner, potentially reducing the risk of perforation, emergency surgery, or unplanned diversion.
This case features the importance of careful patient selection, preprocedural planning, and respect of tissue planes during stricture therapy. Endoscopists can learn how staged interventions, shallow circumferential dissection, and constant reassessment of safety cues can expand the therapeutic envelope of endoscopic stricturotomy. The video also reinforces that not all strictures require aggressive single-session therapy; instead, a graded approach may improve outcomes in complex cases.
Finally, integration of follow-up imaging and preventive measures, such as clip-based stricturoplasty, can help maintain long-term luminal patency. The SLICE technique is not intended to replace conventional approaches, but it serves as an additional option for select complex strictures when appropriate expertise is available. Wider validation and procedural standardization will be important as this approach evolves.
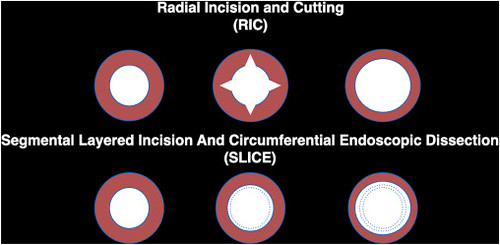
Schematic diagram showing differences between radial incion and cutting (RIC) and segmental layered incision and circumferential endoscopic dissection (SLICE) techniques of endoscopic stricturotomy.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
