
Post written by Shanshan Shen, MD, PhD, from the Department of Gastroenterology, Affiliated Drum Tower Hospital, Medical School of Nanjing University, Nanjing, China.

A 50-year-old woman with refractory vomiting and severe electrolyte imbalance was diagnosed with a cystic-communicating duodenal duplication causing duodenal obstruction. As the patient declined surgical intervention, we performed EUS-guided duodenojejunostomy (EUS-DJ).
Under the guidance of EUS, a 19-gauge needle was used to puncture the jejunum via the duodenal cavity, followed by placement of a 15 × 10-mm lumen-apposing metal stent to establish a duodenojejunal bypass. The patient resumed oral intake by postoperative day 3 and was discharged on day 5. One-month imaging confirmed stent patency and resolution of fluid accumulation. She remained symptom-free at 3-month follow-up.
Duodenal duplication cysts account for 2% to 12% of GI duplications, classified as tubular, cystic-communicating, or cystic-noncommunicating. Although endoscopic management has been reported for noncommunicating cysts, deroofing or excision is generally unsuitable for cystic-communicating types, particularly in cases of large cysts with complex anatomy.
This case illustrates that EUS-DJ is a feasible, minimally invasive, and organ-preserving treatment for cystic-communicating duodenal duplication, particularly in patients with systemic adverse events who are unfit or unwilling to undergo surgery.
Other endoscopists can learn from this experience that EUS-DJ is an effective minimally invasive and feasible option for managing symptomatic duodenal duplication cysts, especially in patients who are poor surgical candidates or who decline surgery.
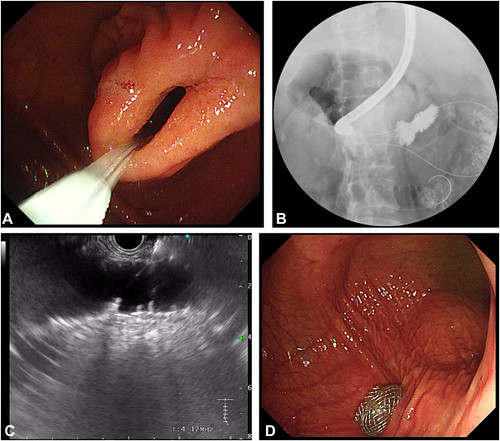
An endoscopic ultrasound (EUS)-guided duodenojejunostomy was performed for duodenal duplication. A, A guidewire was first advanced across the stricture into the distal jejunum. B, Contrast imaging confirmed the distended jejunum after injecting a mixture of methylene blue and sterile water. C, After confirming the puncture site under EUS guidance, we used a 19-gauge needle to puncture the jejunum via the duodenal cavity. D, A 15 × 10-mm lumen-apposing metal stent was used to establish a duodenojejunal bypass.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
