
Post written by Dario Ligresti, MD, from the Digestive Endoscopy Service, Department of Diagnostic and Therapeutic Services, IRCCS-ISMETT, Palermo, Italy, and Radhika Chavan, MD, DNB, FISG, FASGE, from the Department of Gastroenterology and Endoscopy, Bharati Vidyapeeth Medical College, Pune, India.

Our video demonstrates a structured, station-wise approach for identifying liver anatomy during linear EUS. Liver segments are described from 6 stations leveraging anatomical landmarks (ligaments, portal vein branches, hepatic veins, and the inferior vena cava), starting from the gastroesophageal junction and progressing to the duodenal bulb, in order to obtain complete visualization of the liver. Each station correlates EUS views with CT anatomy, enabling systematic visualization of all segments. This video serves as both a learning and reference tool for endosonographers seeking to improve understanding of liver anatomy.
Although EUS is widely used for pancreatic and biliary evaluation, the liver remains an underexplored organ in routine EUS practice. Many trainees find it difficult to orient themselves within hepatic anatomy because of the absence of fixed landmarks and overlapping segments. This video was created to simplify that complexity by presenting a reproducible, structured scanning pathway. It provides an “all-in-1 solution” for learning liver anatomy by offering a real-time correlation of EUS images with cross-sectional imaging and illustrative depictions of scope position and orientation.
Given the expanding scope of endohepatology, incorporating EUS examination of the liver into EUS training programs and routine biliary anatomy evaluation is essential. Through this article, endoscopists can learn how to approach the liver systematically rather than randomly. Understanding liver anatomy with a linear echoendoscope improves image interpretation and increases safety and success of EUS-guided procedures such as biopsies, portal pressure measurements, and targeted therapies.
The liver is emerging as a key focus in diagnostic and therapeutic EUS because of the growing interest in endohepatology. Incorporating liver scanning into every biliopancreatic examination will enhance clinical insight and procedural completeness. As training evolves, one might ask, “Is the liver the new pancreas in routine EUS?” This work suggests it may very well be.
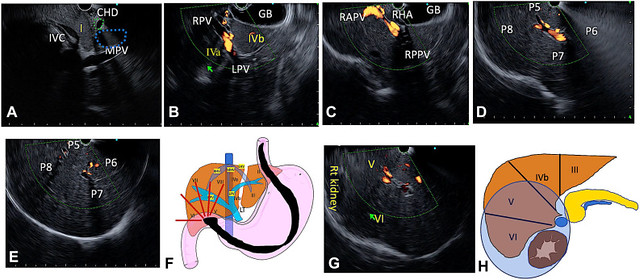
Station 4: Visualization of right segments from the duodenal bulb. A, Follow the main portal vein (MPV) on anticlockwise rotation to the hilum of the liver. EUS image showing common hepatic duct (CHD), inferior vena cava (IVC), and segment I. B, On anticlockwise rotation, the division of MPV into right portal vein (RPV) and left portal vein (LPV) is seen, along with the gallbladder. Segment IVb lies to the right of the LPV, and segment IVa to the left of the LPV. C, Follow the RPV with extreme anticlockwise rotation. The RPV is seen dividing into right anterior portal vein (RAPV) and right posterior portal vein (RPPV). D, On further anticlockwise rotation, branching of the RAPV to the anterior segments (V and VIII) and the posterior (VI and VII) segments are visualized. E, Portal vein branches to the respective segments are traced by further anticlockwise rotation. F, Illustration showing echoendoscope position in duodenal bulb with imaging area. G, On anticlockwise rotation, V and VI are seen along with right kidney. H, Illustration showing imaging area with segments V and VII and right kidney. GB, Gallbladder; LHV, left hepatic vein; MHV, middle hepatic vein; P, portal vein branch; RHA, right hepatic artery; RHV, right hepatic vein.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
