
Post written by Laura Gutiérrez-Rios, MD, Raquel Muñoz-González, MD, and Hugo Uchima, MD, PhD, from the Endoscopy Unit, Gastroenterology Department, Hospital Universitari Germans Trias i Pujol, Badalona, Spain.

This video case series demonstrates the feasibility of cap-suction pseudopolyp formation during underwater EMR for en bloc resection of intra-appendiceal lesions.
Two patients without prior appendectomy were successfully treated using a colonoscope fitted with a conical cap while they were under deep sedation. After complete gas aspiration and saline infusion, the lesions were approached underwater, allowing gentle suction to invaginate them from the appendiceal orifice into the lumen, facilitating en bloc resection. No adverse events occurred. Histology confirmed sessile serrated lesions without dysplasia and R0 resection in both cases.

Intra-appendiceal lesions remain technically challenging for endoscopic resection because of their concealed location and higher risk of incomplete resection. The underwater environment allows the lesion to float into the cap through gentle suction, forming a mucosal/submucosal pseudopolyp.
This maneuver separates these layers from the muscularis propria, reducing the likelihood of deep mural injury or inadvertent full-thickness resection. We felt it was important to share this simple and reproducible approach, as it expands the possibilities for minimally invasive management of appendiceal lesions.

Endoscopists can learn from this experience that en bloc resection of lesions with an intra-appendiceal component is feasible using a straightforward and widely available technique. By applying underwater suction to the intra-appendiceal portion, we create a protruding pseudopolyp, making the lesion easier and safer to capture with a snare.
A conically shaped cap provides optimal suction pressure, although a straight cap also can be used. For effective pseudopolyp formation, the cap should occupy the full appendiceal lumen during underwater suction. Suction must be stopped before snare closure, once the pseudopolyp is fully formed. The underwater milieu should be maintained to ensure that only mucosal and submucosal layers are resected.
During snare closure, careful visual and tactile feedback helps avoid capturing the muscularis propria; warning signs such as abnormal bulging or resistance should prompt immediate release and repositioning. After resection, meticulous inspection and biopsy of the deepest appendiceal margin are recommended to rule out microscopic residual tissue. Clip placement can be performed as a prophylactic plasty of the appendiceal orifice, especially for near-circumferential lesions, to prevent postresection stricture or late appendicitis; we typically attempt to apply 4 clips in a cardinal configuration to preserve luminal patency.
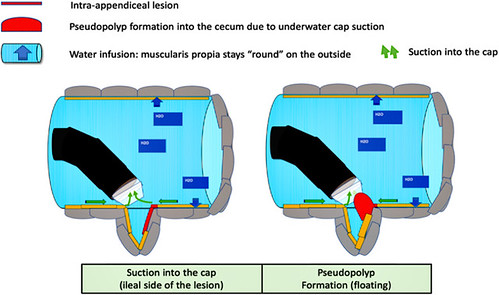
Cap-assisted underwater endoscopic mucosal resection technique. Underwater cap suction is applied, and the lesion prolapses into the cecal as a “pseudopolyp” that floats, making it accessible for endoscopic resection.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
