
Post written by Yohei Nishikawa, MD, PhD, from Digestive Diseases Center, Showa Medical University Koto Toyosu Hospital, Tokyo, Japan.

We present a case of a 56-year-old woman with a recurrent fibrovascular polyp (FVP) in the hypopharynx. She previously underwent an incomplete resection, and the residual tumor continued to grow, leading to progressive dysphagia.
We performed peroral endoscopic tumor resection (POET) with the patient under general anesthesia, combined with special airway management using temporary percutaneous cricothyrotomy and laryngeal expansion with a rigid laryngoscope. En bloc enucleation of the tumor was successfully achieved with a minimal mucosal incision and string-clip traction. The patient recovered well and was discharged without adverse events.
FVPs are rare benign submucosal tumors, but they can cause significant morbidity because of dysphagia or airway obstruction. Traditional surgical approaches may be invasive and technically challenging. By highlighting this case, we wanted to show that POET, when combined with proper airway management techniques, can provide a safe and minimally invasive alternative for treating recurrent hypopharyngeal FVPs.
This case demonstrates the feasibility of adapting POET to treat tumors in anatomically narrow and complex areas such as the hypopharynx. The use of airway protection strategies, including percutaneous cricothyrotomy and laryngeal expansion, can secure a safe operative field while maintaining patient safety. Endoscopists can learn how to combine advanced endoscopic techniques with airway management to achieve complete tumor resection in challenging pharyngeal locations.
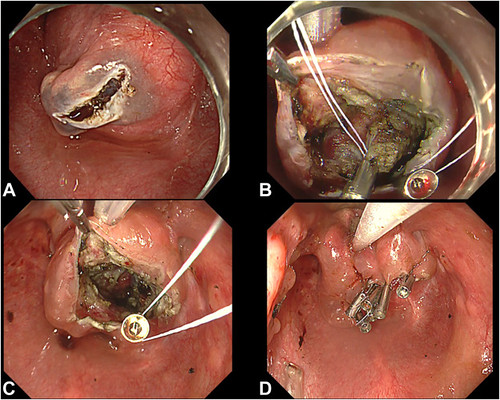
Endoscopic resection. A, A horizontal mucosal incision on the tumor was made. B, After exposing the tumor, we performed the string-clip traction method. Traction was applied at 3 points: both sides of the mucosa and the tumor itself. C, En bloc enucleation was achieved without damaging the tumor surface. D, The mucosal incision site was closed using clips.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
