
Post written by Tatsuma Nomura, MD, from Mie Prefectural Shima Hospital, Shima, Mie, Japan.

We recently developed a new procedure known as full-thickness resection closure using a reopenable-clip over-the-line method inside a submucosal pocket (ROLM-SP) procedure.
During this procedure, the first mucosal incision was made at 20 mm from the center, and a calibrated, small-caliber tip, transparent hood with a 4-mm tapered tip was used to make a small mucosal incision. A submucosal pocket was created, and the surrounding submucosa was dissected while excluding the center part.
All procedures must be performed at low pressure to prevent gas leakage from the stomach wall because of excessive endoscopic insufflation. We used the reopenable-clip over-the-line method for full-thickness defect closure in the pocket.
First, a clip with a line was grasped and placed in the serous muscle layer on the anal side. Next, a reopenable clip with a nylon line threaded through a tooth hole on 1 side was placed in the serous muscle layer—this is the reopenable-clip over-the-line method. Clips with line threaded through the teeth were placed, repeatedly, on the contralateral defect edge. The reopenable clip first grasped the tissue, and subsequently the line started to be pulled.
Then, the clip was placed after confirming endoscopically that the defect edges were close together. The reopenable-clip over-the-line method was repeated, and the full-thickness defect was gradually closed. Once it was completely closed, insufflation was performed to improve the endoscopic view. The remaining mucosa was dissected, and the lesion was resected en bloc, with a long diameter of 40 mm and a full-thickness resection of 20 mm.
A second reopenable-clip over-the-line method was added to the remaining mucosal defect to ensure complete closure. No leakage from the stomach was found, and the procedure time was 79 minutes.
Endoscopic submucosal dissection (ESD) is an endoscopic technique that allows the complete resection of early tumors. A thin submucosal layer exists in gastric tumors with severe ulceration, and the muscle layer is thinning.
Therefore, cutting the muscle side for en bloc resection is necessary, and a safe resection method is desirable. The pocket-creation method provides ideal endoscopic maneuverability inside the submucosal pocket. Thus, we developed ROLM-SP, which we demonstrated in a pig.
Using our ROLM-SP procedure, full-thickness resection can be performed with the pocket-creation method while maintaining low lumen pressure, followed by full-thickness closure of the serous muscle layer. The reopenable-clip over-the-line method is a feasible full-thickness defect closure technique because it does not require a single clip to grasp the bilateral defect edges.
Many endoscopists may think that ROLM-SP is technically difficult. However, if this full-thickness defect closure method can be mastered, full-thickness resection of the GI tract can be performed safely, and the ESD skills of each endoscopist can be improved. ROLM-SP closure can be used for defect closure in a variety of situations, including narrow lumens and GI tracts where maneuverability of the scope is poor.
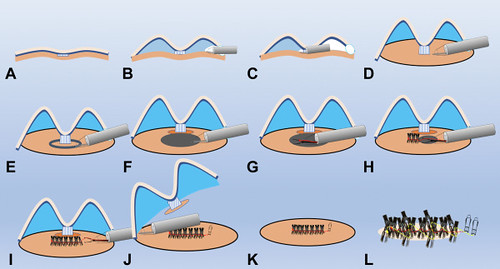
Schema of the reopenable-clip over-the-line method inside a submucosal pocket. A-D, A submucosal pocket is created, and the surrounding submucosa is dissected while excluding the center, creating a protrusion resembling a doughnut. E and F, Full-thickness resection is subsequently performed around the lesion, and the mucosal defect floor is perforated with a long axis of approximately 20 mm. G-I, A clip with a line is grasped and placed in the serous muscle layer on the anal side. Next, a reopenable-clip with a nylon line threaded through a tooth hole on one side is placed in the serous muscle layer (reopenable-clip over-the-line method). Finally, the reopenable-clip over-the-line method is repeated, allowing the full-thickness defect to be completely closed. J, The remaining mucosa is subsequently dissected. K and L, To prevent posterior bleeding, the reopenable-clip over-the-line method is repeated from the anal to the oral side to completely close the full-thickness defect.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
